Toxoplasma gondii Infection(統合失調症.思覺失調症)(双極性障害.躁鬱症)(トキソプラズマ.弓形蟲感染症.Toxoplasma gondii)
還要多少犧牲?毛寶不願面對的真相 トキソプラズマ感染と予防について解説 寄生蟲是如何改變生物體的行為(有字幕.中日字幕あり)
Relationship With Aggression in Psychiatric Subjects
Emil F. Coccaro, MDa,*; Royce Lee, MDa; Maureen W. Groer, PhDb; Adem Can, PhDc; Mary Coussons-Read, PhDd; and Teodor T. Postolache, MDc,e
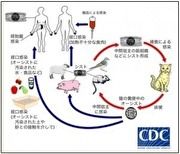
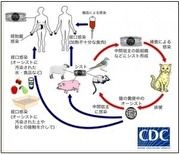
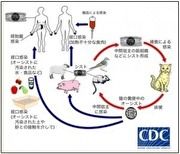
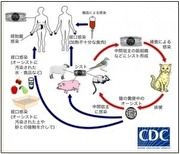
Toxoplasma gondii (T. gondii) is a highly successful neurotropic protozoan parasite, infecting any warm-blooded animal including approximately one-third of all humans.1 Within the animal world, felids have been identified as the definitive host of T. gondii that localizes only in the gastrointestinal tract of any member of the cat family. Humans may be infected by T. gondii via ingestion of the parasite’s oocysts, which can spread from the feces of infected cats. Other routes of transmission include consumption of undercooked meat that has been infected with T. gondii cysts or ingestion of contaminated water2,3; congenital infection, occurring if a mother has a primary infection during pregnancy and transmits T. gondii to the fetus, is relatively rare. Postnatal chronic “latent” infection is very common, minimally symptomatic in the immune competent host, and with an encephalitic picture in the immunocompromised.4 When ingested by an intermediate host, the parasite uses leukocytes to travel from the intestine to other organs, finally localizing in muscle and brain. Once in the brain, T. gondii hides within neurons and glial cells, forming characteristic cystic intracellular structures under the pressure of the immune system.5 Although it is thought to be relatively harmless in immunocompetent adults, latent toxoplasmosis has been linked to several psychiatric disorders (eg, schizophrenia,6,7 bipolar disorder,7–9 personality disorders10) and with suicidal behavior.11–17
Given the strong relationship between suicidal behavior and impulsive aggressive behavior,18 either as a dimension or as a category, and in light of a recent study19 that reported that T. gondii seropositivity status may be associated with high self-reported trait aggression and impulsivity in mentally healthy individuals, we hypothesized that the categorical presence of immunoglobulin G (IgG) antibodies to T. gondii would (1) be associated with higher aggression and impulsivity scores in a sample of psychiatric and healthy control subjects and (2) be more frequent in individuals with intermittent explosive disorder (IED), a disorder of recurrent, problematic, and impulsive aggressive behavior, compared with healthy controls. In this study, we used psychometric assessments20–23 as the dimensional representation of impulsive aggression and the presence of IED as the categorical representation24 of impulsive aggression.
METHOD
Subjects
Three hundred fifty-eight physically healthy subjects participated in this study. All subjects were systematically evaluated in regard to aggressive, anxiety, and other behaviors as part of a larger program that is designed to study correlates of impulsive aggressive and other personality-related behaviors in human subjects. Subjects were recruited through public service, newspaper, and other media announcements seeking individuals who (1) reported psychosocial difficulty related to syndromal psychiatric and/or personality disorder conditions or (2) had little evidence of any psychopathology. All subjects gave informed consent and signed the informed consent document approved by the first author’s (E.F.C.) Institutional Review Board.
Diagnostic Assessment
Syndromal and personality disorder diagnoses were made according to DSM-5 criteria.25 Diagnoses were made using information from (1) the Structured Clinical Interview for DSM-IV Axis I disorders (SCID-I)26 for syndromal disorders and the Structured Interview for DSM-IV Personality (SIDP-IV)27 for personality disorders, (2) a clinical interview by a research psychiatrist, and (3) the review of all other available clinical data. The research diagnostic interviews were conducted by individuals with a master’s or doctor’s degree in clinical psychology, blinded to the study hypothesis. All diagnostic raters went through a rigorous training program that included lectures on DSM diagnoses and rating systems, videos of expert raters conducting SCID-I/SIDP-IV interviews, and practice interviews and ratings until the raters were deemed reliable by the trainer. This process resulted in good to excellent interrater reliabilities (mean ± SE κ = 0.84 ± 0.05; range, 0.79 to 0.93) across anxiety, mood, substance use, impulse control, and personality disorders. Final diagnoses were assigned by team best-estimate consensus procedures28,29 involving research psychiatrists and clinical psychologists as previously described.30 This methodology has been shown to enhance the accuracy of diagnosis over direct interview alone.31 Subjects with a current history of a substance use disorder or a life history of bipolar disorder, schizophrenia (or other psychotic disorder), or mental retardation were excluded from study.
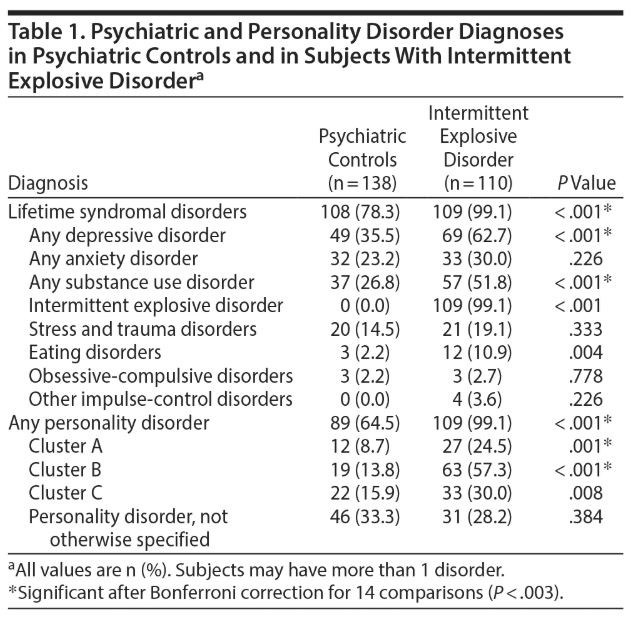
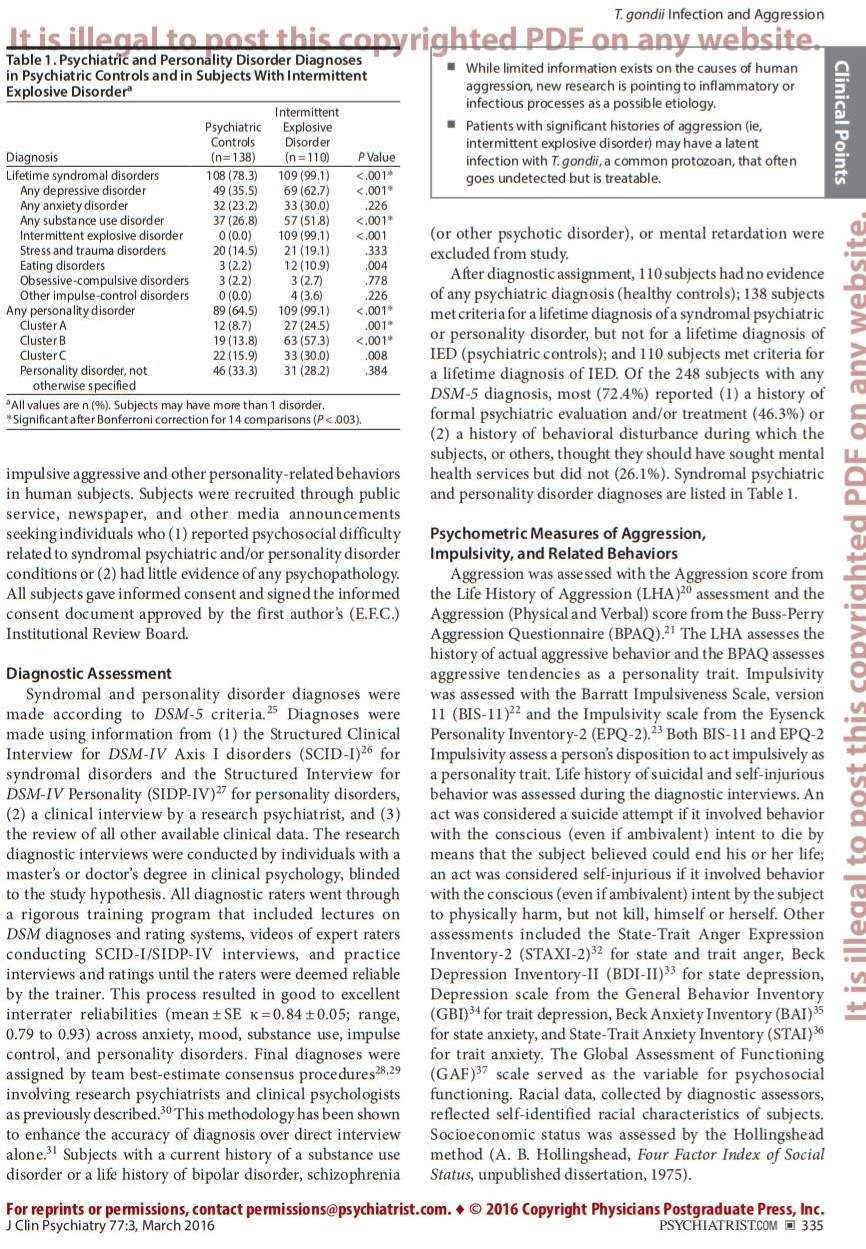
After diagnostic assignment, 110 subjects had no evidence of any psychiatric diagnosis (healthy controls); 138 subjects met criteria for a lifetime diagnosis of a syndromal psychiatric or personality disorder, but not for a lifetime diagnosis of IED (psychiatric controls); and 110 subjects met criteria for a lifetime diagnosis of IED. Of the 248 subjects with any DSM-5 diagnosis, most (72.4%) reported (1) a history of formal psychiatric evaluation and/or treatment (46.3%) or (2) a history of behavioral disturbance during which the subjects, or others, thought they should have sought mental health services but did not (26.1%). Syndromal psychiatric and personality disorder diagnoses are listed in Table 1.
Psychometric Measures of Aggression, Impulsivity, and Related Behaviors
Aggression was assessed with the Aggression score from the Life History of Aggression (LHA)20 assessment and the Aggression (Physical and Verbal) score from the Buss-Perry Aggression Questionnaire (BPAQ).21 The LHA assesses the history of actual aggressive behavior and the BPAQ assesses aggressive tendencies as a personality trait. Impulsivity was assessed with the Barratt Impulsiveness Scale, version 11 (BIS-11)22 and the Impulsivity scale from the Eysenck Personality Inventory-2 (EPQ-2).23 Both BIS-11 and EPQ-2 Impulsivity assess a person’s disposition to act impulsively as a personality trait. Life history of suicidal and self-injurious behavior was assessed during the diagnostic interviews. An act was considered a suicide attempt if it involved behavior with the conscious (even if ambivalent) intent to die by means that the subject believed could end his or her life; an act was considered self-injurious if it involved behavior with the conscious (even if ambivalent) intent by the subject to physically harm, but not kill, himself or herself. Other assessments included the State-Trait Anger Expression Inventory-2 (STAXI-2)32 for state and trait anger, Beck Depression Inventory-II (BDI-II)33 for state depression, Depression scale from the General Behavior Inventory (GBI)34 for trait depression, Beck Anxiety Inventory (BAI)35 for state anxiety, and State-Trait Anxiety Inventory (STAI)36 for trait anxiety. The Global Assessment of Functioning (GAF)37 scale served as the variable for psychosocial functioning. Racial data, collected by diagnostic assessors, reflected self-identified racial characteristics of subjects. Socioeconomic status was assessed by the Hollingshead method (A. B. Hollingshead, Four Factor Index of Social Status, unpublished dissertation, 1975).
Asessment of T. gondii Seropositivity Status
![]()
Subjects were free of all medications for at least 4 weeks. Whole blood, anticoagulated with EDTA (ethylenediaminetetraacetic acid), was obtained between 9 am and 11 am through venipuncture of a forearm vein. Plasma was processed after centrifugation, placed in a polypropylene tube, and stored at −80°C until assay. These frozen plasma samples were collected between 1991 and 2008 and were tested for IgG antibodies to T. gondii in 2014 by solid-phase enzyme-linked immunosorbent assay (ELISA) with kits from IBL (Hamburg, Germany). All samples were run in duplicate, and quality controls were used. The coefficient of intra-assay variation was less than 10%. A subject with plasma T. gondii IgG antibodies > 12 IU was considered to be seropositive for T. gondii. Equivocal samples (8–12 IUs) were reanalyzed to accurately classify them as negative or positive. The laboratory technician was not aware of the diagnostic status of the subject. T. gondii seropositive status, rather than serointensity, was used because the latter cannot be measured in seronegative subjects. Despite the 18-year duration of sample collection, no association was observed between T. gondii seropositive status and time from the first to last study year (Spearman ρ = 0.08, P = .12). Finally, plasma levels for the proinflammatory cytokine interleukin 6 (IL-6) were available in 176 of these subjects as part of a previously published study.38
Statistical Analysis
Comparisons of between-group variables were performed by χ2, univariate (ANOVA/ANCOVA), and multivariate analysis of variance/covariance (MANOVA/MANCOVA), followed by Tukey honestly significant difference post hoc testing. Other analyses included binary logistic regression using age as a covariate. The primary biological variable in this study was T. gondii seropositive status as in previous studies.19 The primary dimensional variables included composite scores for aggression and impulsivity; these variables were created by z-transforming each of the 2 sets of aggression (LHA/BPAQ) and impulsivity (BIS-11/EPQ-2) variables and taking the mean z score of the source variables. The primary categorical variables included diagnostic status (healthy controls/psychiatric controls/subjects with IED), positive history of suicide attempt, and positive history of self-injurious behavior. A 2-tailed α value of .05 was used to denote statistical significance for all analyses. The primary analysis tested the relationship between T. gondii seropositive status and composite aggression scores, composite impulsivity scores, and history of self-directed aggression in all subjects. This was followed by analyses to determine if (1) T. gondii seropositive status was more frequent among IED subjects (subjects characterized by high levels of impulsive aggressive and suicidal behaviors), (2) T. gondii seropositive status was greater among subjects with other psychiatric and personality disorders, and (3) T. gondii seropositive individuals had higher levels of state and/or trait depression, anxiety, or anger.
RESULTS
Demographic Characteristics of the Sample
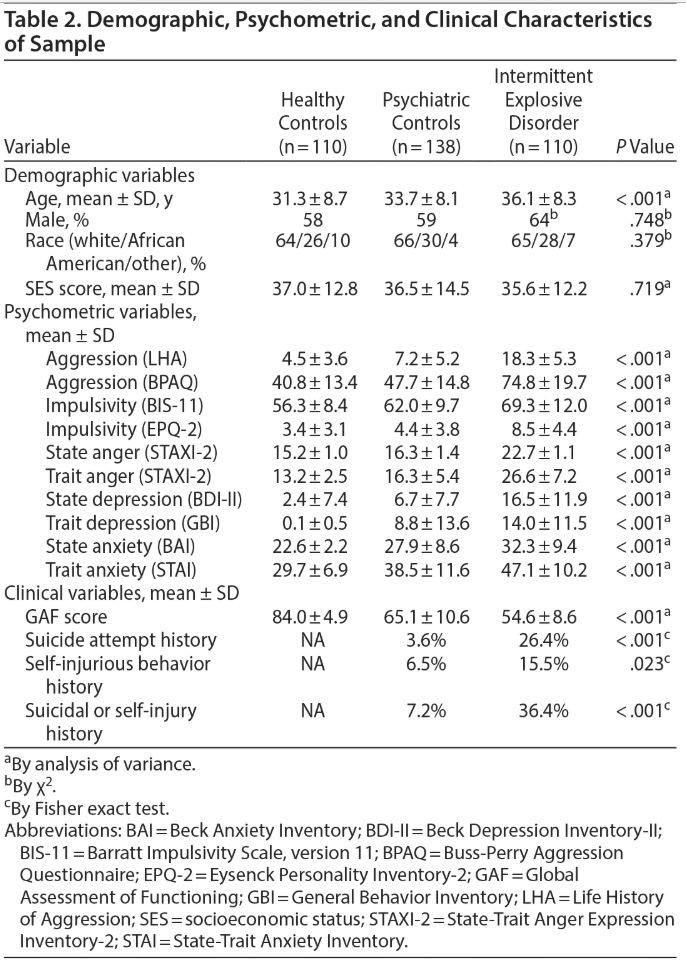
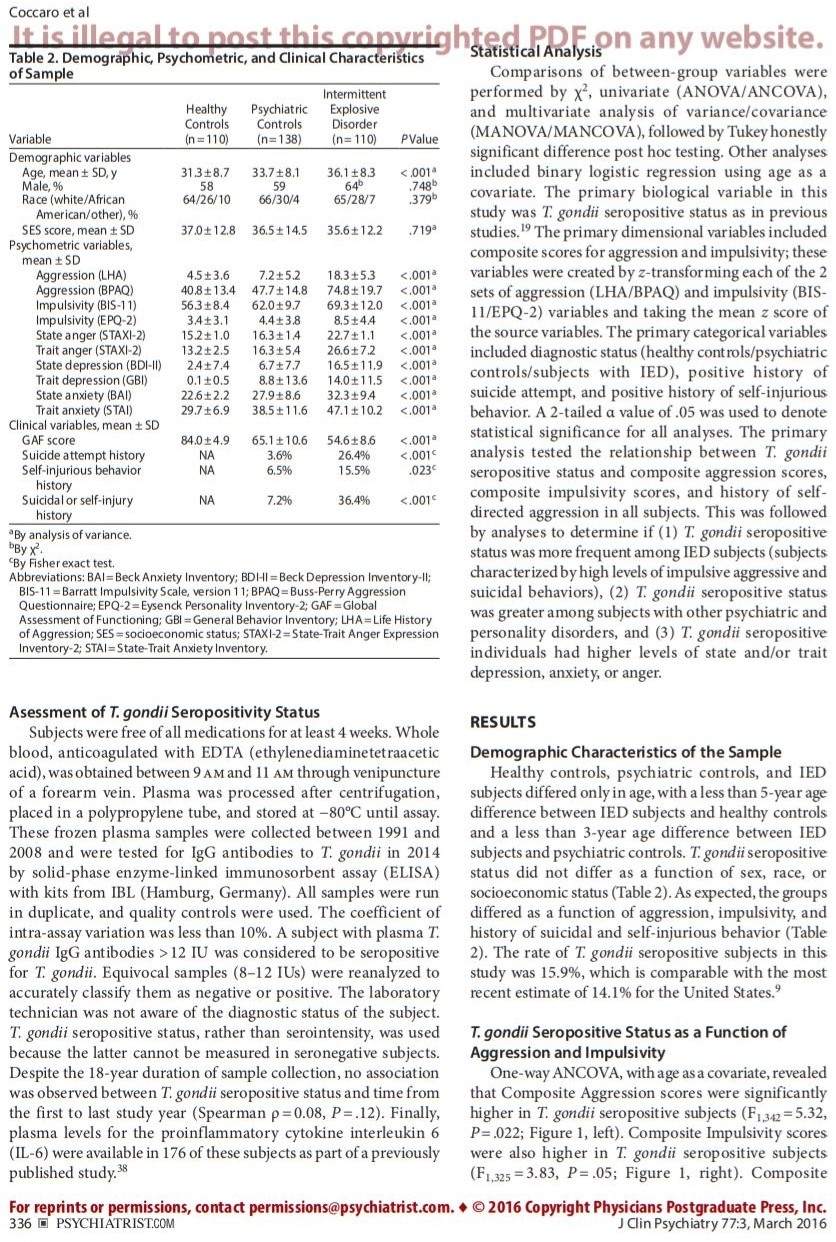
Healthy controls, psychiatric controls, and IED subjects differed only in age, with a less than 5-year age difference between IED subjects and healthy controls and a less than 3-year age difference between IED subjects and psychiatric controls. T. gondii seropositive status did not differ as a function of sex, race, or socioeconomic status (Table 2). As expected, the groups differed as a function of aggression, impulsivity, and history of suicidal and self-injurious behavior (Table 2). The rate of T. gondii seropositive subjects in this study was 15.9%, which is comparable with the most recent estimate of 14.1% for the United States.9
T. gondii Seropositive Status as a Function of Aggression and Impulsivity
![]()
![]()
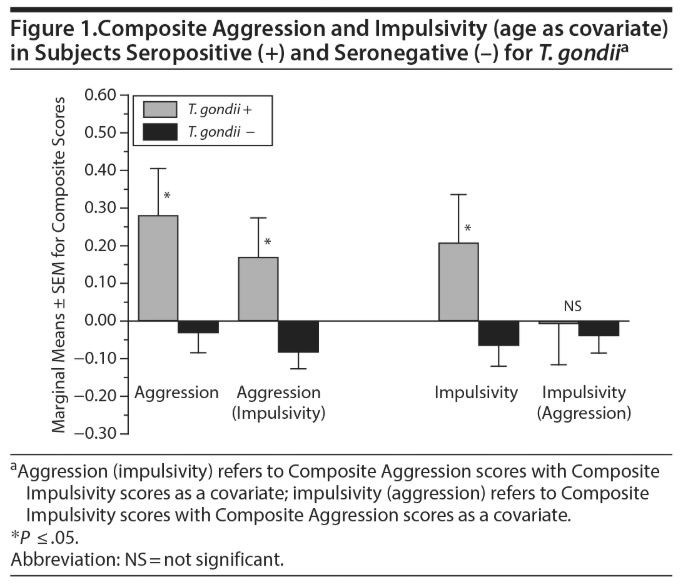
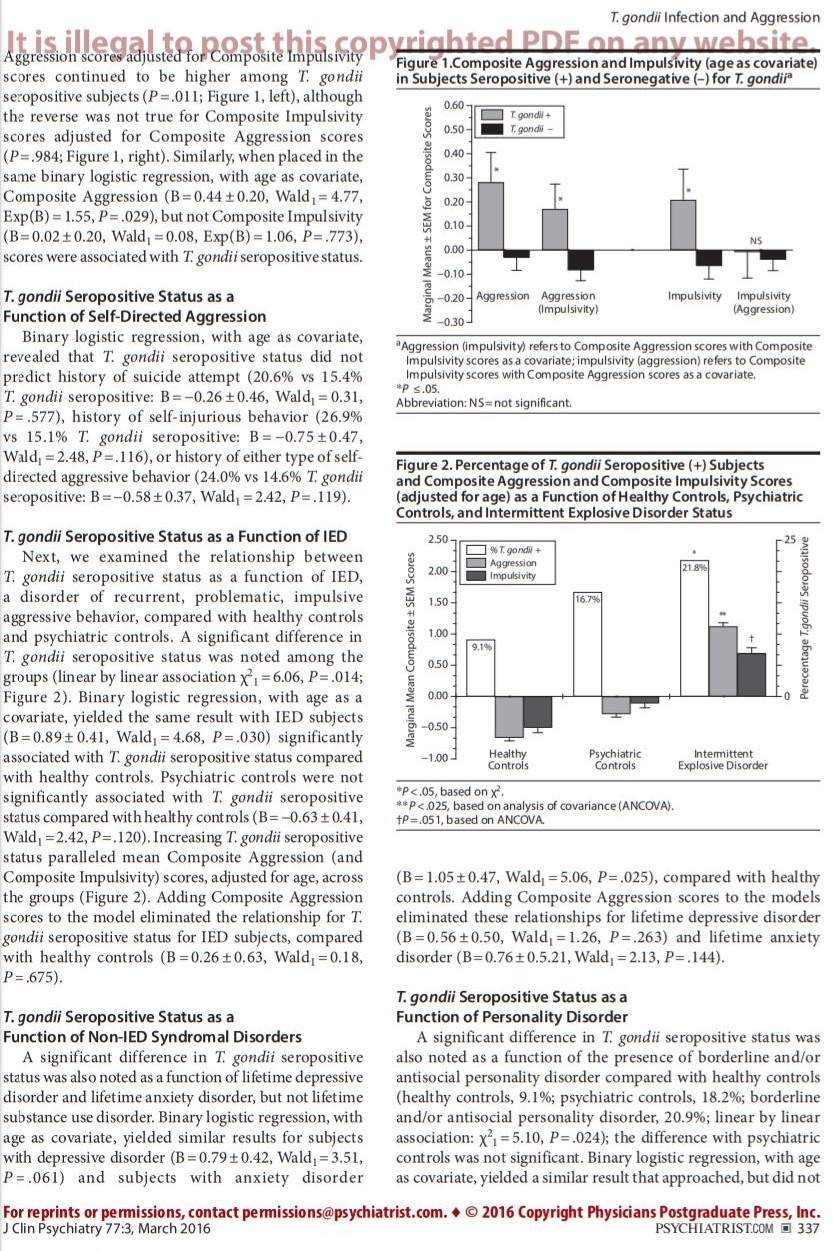
One-way ANCOVA, with age as a covariate, revealed that Composite Aggression scores were significantly higher in T. gondii seropositive subjects (F1,342 = 5.32, P = .022; Figure 1, left). Composite Impulsivity scores were also higher in T. gondii seropositive subjects (F1,325 = 3.83, P = .05; Figure 1, right). Composite Aggression scores adjusted for Composite Impulsivity scores continued to be higher among T. gondii seropositive subjects (P = .011; Figure 1, left), although the reverse was not true for Composite Impulsivity scores adjusted for Composite Aggression scores (P = .984; Figure 1, right). Similarly, when placed in the same binary logistic regression, with age as covariate, Composite Aggression (B = 0.44 ± 0.20, Wald1 = 4.77, Exp(B) = 1.55, P = .029), but not Composite Impulsivity (B = 0.02 ± 0.20, Wald1 = 0.08, Exp(B) = 1.06, P = .773), scores were associated with T. gondii seropositive status.
T. gondii Seropositive Status as a Function of Self-Directed Aggression
![]()
Binary logistic regression, with age as covariate, revealed that T. gondii seropositive status did not predict history of suicide attempt (20.6% vs 15.4% T. gondii seropositive: B = −0.26 ± 0.46, Wald1 = 0.31, P = .577), history of self-injurious behavior (26.9% vs 15.1% T. gondii seropositive: B = −0.75 ± 0.47, Wald1 = 2.48, P = .116), or history of either type of self-directed aggressive behavior (24.0% vs 14.6% T. gondii seropositive: B = −0.58 ± 0.37, Wald1 = 2.42, P = .119).
T. gondii Seropositive Status as a Function of IED
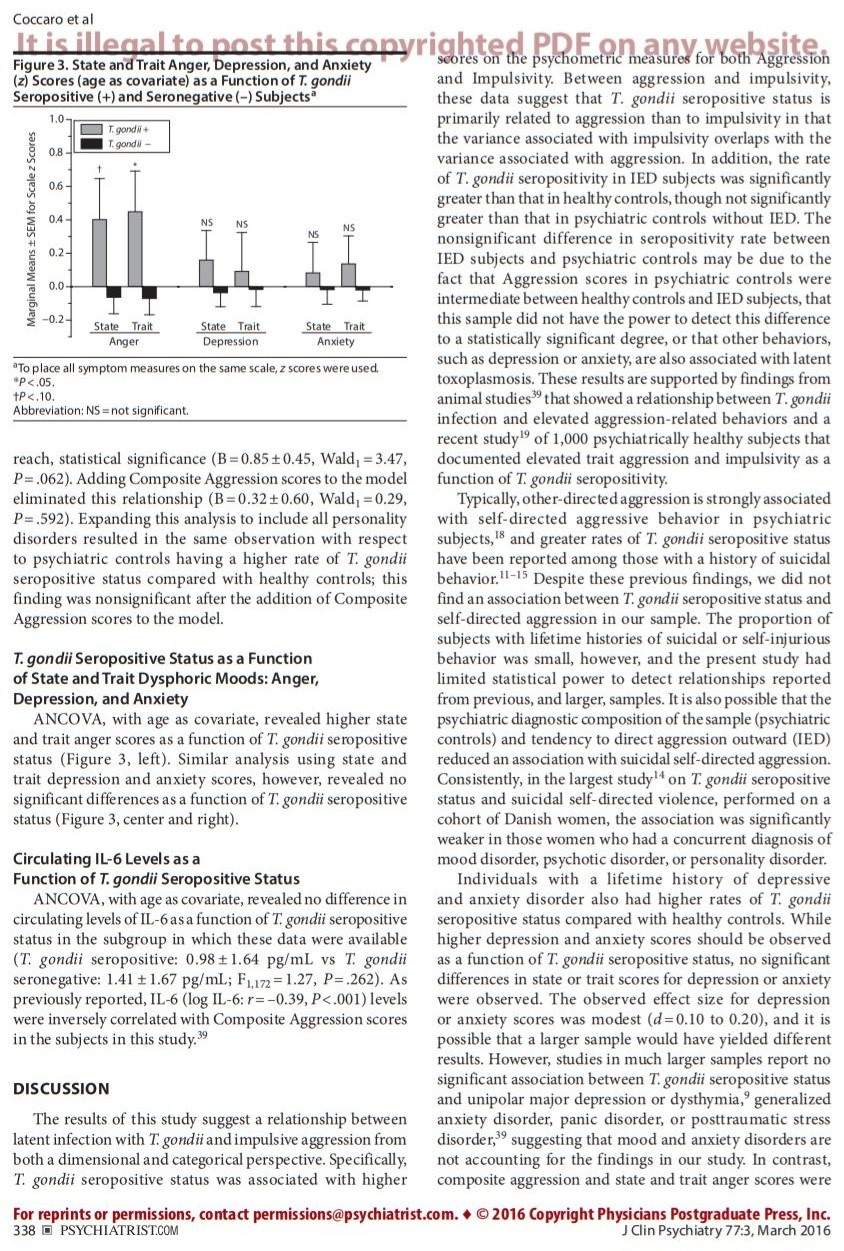
Next, we examined the relationship between T. gondii seropositive status as a function of IED, a disorder of recurrent, problematic, impulsive aggressive behavior, compared with healthy controls and psychiatric controls. A significant difference in T. gondii seropositive status was noted among the groups (linear by linear association χ21 = 6.06, P = .014; Figure 2). Binary logistic regression, with age as a covariate, yielded the same result with IED subjects (B = 0.89 ± 0.41, Wald1 = 4.68, P = .030) significantly associated with T. gondii seropositive status compared with healthy controls. Psychiatric controls were not significantly associated with T. gondii seropositive status compared with healthy controls (B = −0.63 ± 0.41, Wald1 = 2.42, P = .120). Increasing T. gondii seropositive status paralleled mean Composite Aggression (and Composite Impulsivity) scores, adjusted for age, across the groups (Figure 2). Adding Composite Aggression scores to the model eliminated the relationship for T. gondii seropositive status for IED subjects, compared with healthy controls (B = 0.26 ± 0.63, Wald1 = 0.18, P = .675).
T. gondii Seropositive Status as a Function of Non-IED Syndromal Disorders
A significant difference in T. gondii seropositive status was also noted as a function of lifetime depressive disorder and lifetime anxiety disorder, but not lifetime substance use disorder. Binary logistic regression, with age as covariate, yielded similar results for subjects with depressive disorder (B = 0.79 ± 0.42, Wald1 = 3.51, P = .061) and subjects with anxiety disorder (B = 1.05 ± 0.47, Wald1 = 5.06, P = .025), compared with healthy controls. Adding Composite Aggression scores to the models eliminated these relationships for lifetime depressive disorder (B = 0.56 ± 0.50, Wald1 = 1.26, P = .263) and lifetime anxiety disorder (B = 0.76 ± 0.5.21, Wald1 = 2.13, P = .144).
T. gondii Seropositive Status as a Function of Personality Disorder
A significant difference in T. gondii seropositive status was also noted as a function of the presence of borderline and/or antisocial personality disorder compared with healthy controls (healthy controls, 9.1%; psychiatric controls, 18.2%; borderline and/or antisocial personality disorder, 20.9%; linear by linear association: χ21 = 5.10, P = .024); the difference with psychiatric controls was not significant. Binary logistic regression, with age as covariate, yielded a similar result that approached, but did not reach, statistical significance (B = 0.85 ± 0.45, Wald1 = 3.47, P = .062). Adding Composite Aggression scores to the model eliminated this relationship (B = 0.32 ± 0.60, Wald1 = 0.29, P = .592). Expanding this analysis to include all personality disorders resulted in the same observation with respect to psychiatric controls having a higher rate of T. gondii seropositive status compared with healthy controls; this finding was nonsignificant after the addition of Composite Aggression scores to the model.
T. gondii Seropositive Status as a Function of State and Trait Dysphoric Moods: Anger, Depression, and Anxiety
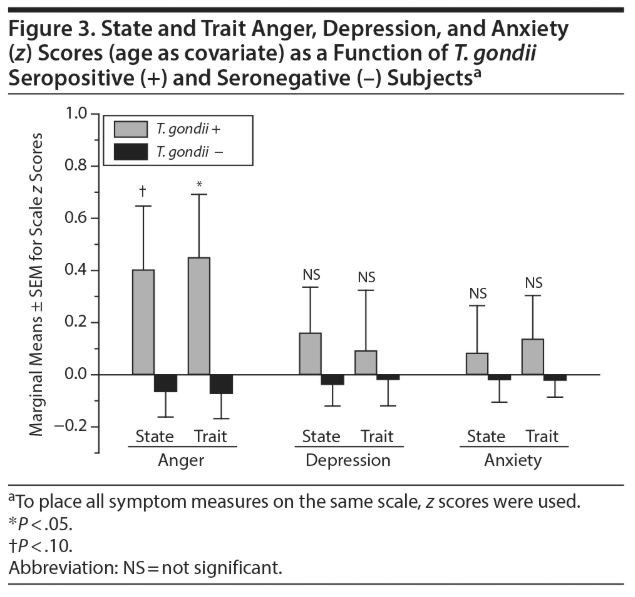
ANCOVA, with age as covariate, revealed higher state and trait anger scores as a function of T. gondii seropositive status (Figure 3, left). Similar analysis using state and trait depression and anxiety scores, however, revealed no significant differences as a function of T. gondii seropositive status (Figure 3, center and right).
Circulating IL-6 Levels as a Function of T. gondii Seropositive Status
![]()
ANCOVA, with age as covariate, revealed no difference in circulating levels of IL-6 as a function of T. gondii seropositive status in the subgroup in which these data were available (T. gondii seropositive: 0.98 ± 1.64 pg/mL vs T. gondii seronegative: 1.41 ± 1.67 pg/mL; F1,172 = 1.27, P = .262). As previously reported, IL-6 (log IL-6: r = –0.39, P < .001) levels were inversely correlated with Composite Aggression scores in the subjects in this study.39
DISCUSSION
The results of this study suggest a relationship between latent infection with T. gondii and impulsive aggression from both a dimensional and categorical perspective. Specifically, T. gondii seropositive status was associated with higher scores on the psychometric measures for both Aggression and Impulsivity. Between aggression and impulsivity, these data suggest that T. gondii seropositive status is primarily related to aggression than to impulsivity in that the variance associated with impulsivity overlaps with the variance associated with aggression. In addition, the rate of T. gondii seropositivity in IED subjects was significantly greater than that in healthy controls, though not significantly greater than that in psychiatric controls without IED. The nonsignificant difference in seropositivity rate between IED subjects and psychiatric controls may be due to the fact that Aggression scores in psychiatric controls were intermediate between healthy controls and IED subjects, that this sample did not have the power to detect this difference to a statistically significant degree, or that other behaviors, such as depression or anxiety, are also associated with latent toxoplasmosis. These results are supported by findings from animal studies39 that showed a relationship between T. gondii infection and elevated aggression-related behaviors and a recent study19 of 1,000 psychiatrically healthy subjects that documented elevated trait aggression and impulsivity as a function of T. gondii seropositivity.
Typically, other-directed aggression is strongly associated with self-directed aggressive behavior in psychiatric subjects,18 and greater rates of T. gondii seropositive status have been reported among those with a history of suicidal behavior.11–15 Despite these previous findings, we did not find an association between T. gondii seropositive status and self-directed aggression in our sample. The proportion of subjects with lifetime histories of suicidal or self-injurious behavior was small, however, and the present study had limited statistical power to detect relationships reported from previous, and larger, samples. It is also possible that the psychiatric diagnostic composition of the sample (psychiatric controls) and tendency to direct aggression outward (IED) reduced an association with suicidal self-directed aggression. Consistently, in the largest study14 on T. gondii seropositive status and suicidal self-directed violence, performed on a cohort of Danish women, the association was significantly weaker in those women who had a concurrent diagnosis of mood disorder, psychotic disorder, or personality disorder.
Individuals with a lifetime history of depressive and anxiety disorder also had higher rates of T. gondii seropositive status compared with healthy controls. While higher depression and anxiety scores should be observed as a function of T. gondii seropositive status, no significant differences in state or trait scores for depression or anxiety were observed. The observed effect size for depression or anxiety scores was modest (d = 0.10 to 0.20), and it is possible that a larger sample would have yielded different results. However, studies in much larger samples report no significant association between T. gondii seropositive status and unipolar major depression or dysthymia,9 generalized anxiety disorder, panic disorder, or posttraumatic stress disorder,39 suggesting that mood and anxiety disorders are not accounting for the findings in our study. In contrast, composite aggression and state and trait anger scores were significantly elevated as a function of T. gondii seropositive status and, in every case, eliminated all differences as a function of T. gondii seropositive status. Thus, we posit that the higher T. gondii seropositive rates observed in individuals with depressive/anxiety disorder, compared with healthy controls, were due to their comorbidity with IED or a correlation between aggression, depression, and anxiety scores. In the current sample, IED was highly comorbid with lifetime depressive disorder (64% vs 35%, P < .001), and aggression scores correlated with both trait depression (r = 0.38, P = .001) and anxiety (r = 0.52, P < .001) scores, though not as strongly as depression correlated with anxiety (r = 0.74, P < .001).
Several factors may account for these findings. First, chronic latent infection with T. gondii may lead to a low-grade chronic immune activation within the brain, with (or without) downstream effects on neurotransmitter systems involved in aggressive behavior.40 Second, chronic T. gondii infection may alter the structure and function of corticolimbic circuits that are known to modulate impulsive aggressive behavior.41 Specifically, persistent T. gondii infection in mice is associated with neuronal tissue lesions, altered neuronal function, ventricular dilation, and neuroinflammation.42 In addition, several, though not all, studies suggest that T. gondii–containing cysts localize primarily in the prefrontal cortex and amygdala43,44 and that latent infection with T. gondii induces dendritic retraction in the basolateral amygdala.45 Third, as shown experimentally in rats,46 T. gondii infection increases testicular expression of genes involved in the production of testosterone. In addition, there is evidence that T. gondii–infected males, though not females, have higher circulating levels of testosterone compared with controls.47 However, while a number of studies report a relationship between elevated levels of testosterone and aggression,48 the magnitude of this relationship is small. Thus, it is unlikely that testosterone plays any more than a modest role in this regard.
Neurotransmitter mechanisms by which T. gondii may affect behavior include effects on serotonergic and glutaminergic transmission, both of which have been shown to play a role in aggressive behavior in human studies.49,50 Relevant to serotonin, conversion of tryptophan to kynurenine is controlled by indoleamine 2,3-dioxygenase ([IDO]; IDO-1 and IDO-2).51 Since IDO can be activated by inflammatory cytokines, levels of kynurenine can rise while levels of serotonin decline. In addition, increased levels of kynurenine lead to increased levels of its active metabolite quinolinic acid, a potent N-methyl-d-aspartate receptor agonist, which may increase the risk for aggressive behavior in humans.50 While this hypothesis is partially supported by reported elevations of kynurenine and quinolinic acid levels in mice with chronic T. gondii infection,52 we did not find differences in circulating levels of proinflammatory cytokines (ie, IL-6) as a function of T. gondii seropositivity. It is possible that the proinflammatory processes that keep T. gondii in a latent state are confined to the brain and are not reflected in the periphery. It is also possible that impulsively aggressive individuals engage in behaviors that increase their own risk of infection with T. gondii or that latent toxoplasmosis changes behavior, as in felids,1 so that the expression of aggression is increased. In addition, T. gondii is known to increase risk-taking behavior in rodents, evolutionarily benefiting the parasite (ie, transforming natural aversion in cats to attraction).53,54 This is an example of the general phenomenon of host manipulation by parasites, documented in nature,55 and proposed as a model with some explanatory potential for alterations in human behavior associated with parasitic infections.56,57
The strengths of this hypothesis-driven study include a well-characterized sample of healthy and psychiatric controls as well as validated measures of aggression, impulsivity, depression, and anxiety. Limitations to our study are present, as well. First, we used a cross-sectional design, and no causal, or directional, conclusions can be made from these analyses. Second, ascertainment of subjects may limit the generalizability of these findings in that these involved subjects who volunteered for a research study, rather than for clinical treatment. However, nearly three-quarters of the psychiatric subjects reported a past history of psychiatric treatment (or of having episodes of behavioral disturbance for which they, or others, thought they should have sought mental health services but did not), and, thus, most of these subjects are likely similar to individuals who would have been recruited from a clinical setting. Third, it is possible that the presented associations are nonspecific and, instead, due to other common latency-establishing neurotropic pathogens such as herpes viruses or cytomegalovirus. However, recent studies have documented that associations between T. gondii and self-directed58 and other-directed19 aggression in human subjects are not due to the presence of these other potential pathogens. Finally, because immunoglobulin M antibodies to T. gondii were not assessed, there is a possibility that a small number of seropositive subjects had an acute, rather than a chronic latent, infection at time of study.
In summary, we report a greater rate of T. gondii seropositive status in subjects with DSM-5 IED compared with healthy controls and a positive relationship with aggression and anger, but not with depression or anxiety. These findings are consistent with previous T. gondii seropositive status data, suggesting a relationship with self-directed aggression (ie, suicidal behavior) and a relationship involving schizophrenia or mania—disorders in which many individuals are often aggressive.59,60 Our results further add to the biological complexity of impulsive aggression, from both a categorical and a dimensional perspective.
Submitted: October 29, 2014; accepted February 26, 2015.
Potential conflicts of interest: Dr Coccaro reports being a consultant and on the Scientific Advisory Board of and having stock options from Azevan Pharmaceuticals. Dr Lee reports being the recipient of a research grant from Azevan Pharmaceuticals. Drs Groer, Can, Coussons-Read, and Postolache have no potential conflicts of interest.
Funding/support: This work was supported, in part, by grants from the National Institute of Mental Health: RO1 MH60836, RO1 MH63262, RO1 MH66984 (Dr Coccaro), a Project Pilot Grant from the University of Colorado, Denver (Dr Coussons-Read), and the Distinguished Investigator Award from the American Foundation for Suicide Prevention (Dr Postolache). Dr Postolache’s contribution was additionally supported by the Veterans Integrated Service Network 19 Mental Illness Research, Education and Clinical Center, Denver, Colorado.
Role of the sponsor: The funding agencies had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, and approval of the manuscript.
Disclaimer: The views, opinions, and findings contained in this article are those of the authors and do not necessarily represent the official policy or position of the Department of Veterans Affairs or the US Government.
While limited information exists on the causes of human aggression, new research is pointing to inflammatory or infectious processes as a possible etiology.
Patients with significant histories of aggression (ie, intermittent explosive disorder) may have a latent infection with T. gondii, a common protozoan, that often goes undetected but is treatable.
ABSTRACT
Objective: Toxoplasma gondii (T. gondii), a protozoan parasite that persists in host tissues, including brain, has been associated with several psychiatric disorders and with suicidal behavior. We sought to test the hypothesis that latent T. gondii infection, as manifest by circulating immunoglobulin G (IgG) antibodies to T. gondii, is associated with both categorical and dimensional measures of aggression.
Method: IgG antibodies to T. gondii were collected between 1991 and 2008 from 358 adult subjects with DSM-5 intermittent explosive disorder (IED), non-IED psychiatric disorders (psychiatric controls), or no evidence of any psychiatric diagnosis (healthy controls). Assessments of aggression, anger, and impulsivity, as well as state/trait anger, depression, and anxiety were completed. T. gondii seropositive status (IgG > 12 IU) was the primary outcome measure for this study.
Results: T. gondii seropositive status (IgG > 12 IU) was associated with higher aggression (P = .022) and impulsivity (P = .05) scores. When both aggression and impulsivity scores were controlled for, however, only aggression scores were higher in seropositive subjects (P = .011). In addition, T. gondii seropositive status and marginal mean ± SE aggression scores increased from healthy controls (9.1% and −0.66 ± 0.05) to psychiatric controls (16.7% and −0.27 ± 0.05) to subjects with IED (21.8% and 1.15 ± 0.06; P ≤ .05). These findings were not accounted for by the presence of other syndromal/personality disorders or by states or traits related to depressed or anxious moods.
Conclusions: These data are consistent with previous studies suggesting a relationship between T. gondii and self-directed aggression (ie, suicidal behavior) and further add to the biological complexity of impulsive aggression both from a categorical and a dimensional perspective.
J Clin Psychiatry 2016;77(3):334–341
https://doi.org/10.4088/JCP.14m09621
© Copyright 2016 Physicians Postgraduate Press, Inc.
aClinical Neuroscience Research Unit, Department of Psychiatry and Behavioral Neuroscience, Pritzker School of Medicine, University of Chicago, Illinois
bCollege of Nursing, University of South Florida, Tampa
cDepartment of Psychiatry, University of Maryland College of Medicine, Baltimore
dDepartment of Psychology, University of Denver, Colorado Springs, Colorado
eVeterans Integrated Service Network 19, Mental Illness Research Education and Clinical Center, Denver, Colorado, and Veterans Integrated Service Network 5, Mental Illness Research Education and Clinical Center, Baltimore, Maryland
*Corresponding author: Emil F. Coccaro, MD, Department of Psychiatry and Behavioral Neuroscience, University of Chicago, 5841 South Maryland Ave, Chicago, IL 60637 (ecoccaro@yoda.bsd.uchicago.edu).
1. Dubey JP, Jones JL. Toxoplasma gondii infection in humans and animals in the United States. Int J Parasitol. 2008;38(11):1257–1278. PubMed doi:10.1016/j.ijpara.2008.03.007 Show Abstract
2. Jones JL, Dargelas V, Roberts J, et al. Risk factors for Toxoplasma gondii infection in the United States. Clin Infect Dis. 2009;49(6):878–884. PubMed doi:10.1086/605433 Show Abstract
3. Jones JL, Kruszon-Moran D, Wilson M, et al. Toxoplasma gondii infection in the United States: seroprevalence and risk factors. Am J Epidemiol. 2001;154(4):357–365. PubMed doi:10.1093/aje/154.4.357 Show Abstract
4. Ajioka JW, Soldati D. Toxoplasma: Molecular and Cellular Biology. Norfolk, UK: Horizon Bioscience; 2007.
5. Garcia SL, Bruckner AD. Parasitic infections in the compromised host (Toxoplasma gondii). In: Garcia S, Bruckner AD, eds. Diagnostic Medical Parasitology. Washingtion, DC: American Society for Microbiology; 1997:423–424.
6. Prasad KM, Watson AM, Dickerson FB, et al. Exposure to herpes simplex virus type 1 and cognitive impairments in individuals with schizophrenia. Schizophr Bull. 2012;38(6):1137–1148. PubMed doi:10.1093/schbul/sbs046 Show Abstract
7. Torrey EF, Bartko JJ, Yolken RH. Toxoplasma gondii and other risk factors for schizophrenia: an update. Schizophr Bull. 2012;38(3):642–647. PubMed doi:10.1093/schbul/sbs043 Show Abstract
8. Tedla Y, Shibre T, Ali O, et al. Serum antibodies to Toxoplasma gondii and Herpesvidae family viruses in individuals with schizophrenia and bipolar disorder: a case-control study. Ethiop Med J. 2011;49(3):211–220. PubMed Show Abstract
9. Pearce BD, Kruszon-Moran D, Jones JL. The relationship between Toxoplasma gondii infection and mood disorders in the third National Health and Nutrition Survey. Biol Psychiatry. 2012;72(4):290–295. PubMed doi:10.1016/j.biopsych.2012.01.003 Show Abstract
10. Hinze-Selch D, Däubener W, Erdag S, et al. The diagnosis of a personality disorder increases the likelihood for seropositivity to Toxoplasma gondii in psychiatric patients. Folia Parasitol (Praha). 2010;57(2):129–135. PubMed doi:10.14411/fp.2010.016 Show Abstract
11. Arling TA, Yolken RH, Lapidus M, et al. Toxoplasma gondii antibody titers and history of suicide attempts in patients with recurrent mood disorders. J Nerv Ment Dis. 2009;197(12):905–908. PubMed doi:10.1097/NMD.0b013e3181c29a23 Show Abstract
12. Okusaga O, Langenberg P, Sleemi A, et al. Toxoplasma gondii antibody titers and history of suicide attempts in patients with schizophrenia. Schizophr Res. 2011;133(1–3):150–155. PubMed doi:10.1016/j.schres.2011.08.006 Show Abstract
13. Yagmur F, Yazar S, Temel HO, et al. May Toxoplasma gondii increase suicide attempt-preliminary results in Turkish subjects? Forensic Sci Int. 2010;199(1–3):15–17. PubMed doi:10.1016/j.forsciint.2010.02.020 Show Abstract
14. Pedersen MG, Mortensen PB, Norgaard-Pedersen B, et al. Toxoplasma gondii infection and self-directed violence in mothers. Arch Gen Psychiatry. 2012;69(11):1123–1130. PubMed doi:10.1001/archgenpsychiatry.2012.668 Show Abstract
15. Ling VJ, Lester D, Mortensen PB, et al. Toxoplasma gondii seropositivity and suicide rates in women. J Nerv Ment Dis. 2011;199(7):440–444. PubMed doi:10.1097/NMD.0b013e318221416e Show Abstract
16. Samojłowicz D, Borowska-Solonynko A, Gołab E. Prevalence of Toxoplasma gondii parasite infection among people who died due to sudden death in the capital city of Warsaw and its vicinity. Przegl Epidemiol. 2013;67(1):29–33, 115–118. PubMed Show Abstract
17. Alvarado-Esquivel C, Sánchez-Anguiano LF, Arnaud-Gil CA, et al. Toxoplasma gondii infection and suicide attempts: a case-control study in psychiatric outpatients. J Nerv Ment Dis. 2013;201(11):948–952. PubMed doi:10.1097/NMD.0000000000000037 Show Abstract
18. McCloskey MS, Ben-Zeev D, Lee R, et al. Prevalence of suicidal and self-injurious behavior among subjects with intermittent explosive disorder. Psychiatry Res. 2008;158(2):248–250. PubMed doi:10.1016/j.psychres.2007.09.011 Show Abstract
19. Cook TB, Brenner LA, Cloninger CR, et al. “Latent” infection with Toxoplasma gondii: association with trait aggression and impulsivity in healthy adults. J Psychiatr Res. 2015;60:87–94. PubMed doi:10.1016/j.jpsychires.2014.09.019 Show Abstract
20. Coccaro EF, Berman ME, Kavoussi RJ. Assessment of Life History of Aggression: development and psychometric characteristics. Psychiatry Res. 1997;73(3):147–157. PubMed doi:10.1016/S0165-1781(97)00119-4 Show Abstract
21. Buss AH, Perry M. The Aggression Questionnaire. J Pers Soc Psychol. 1992;63(3):452–459. PubMed doi:10.1037/0022-3514.63.3.452 Show Abstract
22. Patton JH, Stanford MS, Barratt ES. Factor structure of the Barratt Impulsiveness Scale. J Clin Psychol. 1995;51(6):768–774. PubMed doi:10.1002/1097-4679(199511)51:6<768::AID-JCLP2270510607>3.0.CO;2-1 Show Abstract
23. Eysenck H Jr, Eysenck SBG. Manual of the Eysenck Personality Scales (EPS Adult). London, UK: Hodder & Stoughton; 1991.
24. Coccaro EF. Intermittent explosive disorder as a disorder of impulsive aggression for DSM-5. Am J Psychiatry. 2012;169(6):577–588. PubMed doi:10.1176/appi.ajp.2012.11081259 Show Abstract
25. American Association of Psychiatry. Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Washington, DC: American Pyschiatric Press, Inc; 2013.
26. First MB, Spitzer RL, Gibbon M, et al. Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I). New York, NY: Psychiatric Institute, Biometrics Research; 1997.
27. Pfohl B, Blum N, Zimmerman M, University of Iowa, Department of Psychiatry. Structured Interview for DSM-IV Personality: SIDP-IV. Washington, DC: American Psychiatric Press; 1997.
28. Kosten TA, Rounsaville BJ. Sensitivity of psychiatric diagnosis based on the best estimate procedure. Am J Psychiatry. 1992;149(9):1225–1227. PubMed doi:10.1176/ajp.149.9.1225 Show Abstract
29. Leckman JF, Sholomskas D, Thompson WD, et al. Best estimate of lifetime psychiatric diagnosis: a methodological study. Arch Gen Psychiatry. 1982;39(8):879–883. PubMed doi:10.1001/archpsyc.1982.04290080001001 Show Abstract
30. Coccaro EF, Nayyer H, McCloskey MS. Personality disorder—not otherwise specified evidence of validity and consideration for DSM-5. Compr Psychiatry. 2012;53(7):907–914. PubMed doi:10.1016/j.comppsych.2012.03.007 Show Abstract
31. Klein DN, Ouimette PC, Kelly HS, et al. Test-retest reliability of team consensus best-estimate diagnoses of axis I and II disorders in a family study. Am J Psychiatry. 1994;151(7):1043–1047. PubMed doi:10.1176/ajp.151.7.1043 Show Abstract
32. Spielberger CD. The State-Trait Anger Expression Inventory-2 (STAXI-2): Professional Manual. Lutz, FL: Psychological Assessment Resources, Inc.; 1999.
33. Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation. 1996.
34. Depue RA, Kleiman RM, Davis P, et al. The behavioral high-risk paradigm and bipolar affective disorder, VIII: serum free cortisol in nonpatient cyclothymic subjects selected by the General Behavior Inventory. Am J Psychiatry. 1985;142(2):175–181. PubMed doi:10.1176/ajp.142.2.175 Show Abstract
35. Beck AT, Epstein N, Brown G, et al. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988;56(6):893–897. PubMed doi:10.1037/0022-006X.56.6.893 Show Abstract
36. Spielberger CD, Gorssuch RL, Lushene PR, et al. Manual for the State-Trait Anxiety Inventory. Mountain View, CA: Consulting Psychologists Press, Inc.; 1983.
37. American Psychiatric Association. Diagnostic and Statistical Manual for Mental Disorders. Fourth Edition, Text Revision. Washington, DC: American Psychiatric Association; 2000.
38. Coccaro EF, Lee R, Coussons-Read M. Elevated plasma inflammatory markers in individuals with intermittent explosive disorder and correlation with aggression in humans. JAMA Psychiatry. 2014;71(2):158–165. PubMed doi:10.1001/jamapsychiatry.2013.3297 Show Abstract
39. Gale SD, Brown BL, Berrett A, et al. Association between latent toxoplasmosis and major depression, generalised anxiety disorder and panic disorder in human adults. Folia Parasitol (Praha). 2014;61(4):285–292. PubMed Show Abstract
40. Flegr J. How and why Toxoplasma makes us crazy. Trends Parasitol. 2013;29(4):156–163. PubMed doi:10.1016/j.pt.2013.01.007 Show Abstract
41. Coccaro EF, Sripada CS, Yanowitch RN, et al. Corticolimbic function in impulsive aggressive behavior. Biol Psychiatry. 2011;69(12):1153–1159. PubMed doi:10.1016/j.biopsych.2011.02.032 Show Abstract
42. Hermes G, Ajioka JW, Kelly KA, et al. Neurological and behavioral abnormalities, ventricular dilatation, altered cellular functions, inflammation, and neuronal injury in brains of mice due to common, persistent, parasitic infection. J Neuroinflammation. 2008;5(1):48. PubMed doi:10.1186/1742-2094-5-48 Show Abstract
43. Berenreiterová M, Flegr J, Kuběna AA, et al. The distribution of Toxoplasma gondii cysts in the brain of a mouse with latent toxoplasmosis: implications for the behavioral manipulation hypothesis. PLoS ONE. 2011;6(12):e28925. PubMed doi:10.1371/journal.pone.0028925 Show Abstract
44. McConkey GA, Martin HL, Bristow GC, et al. Toxoplasma gondii infection and behaviour - location, location, location? J Exp Biol. 2013;216(pt 1):113–119. PubMed doi:10.1242/jeb.074153 Show Abstract
45. Mitra R, Sapolsky RM, Vyas A. Toxoplasma gondii infection induces dendritic retraction in basolateral amygdala accompanied by reduced corticosterone secretion. Dis Model Mech. 2013;6(2):516–520. PubMed doi:10.1242/dmm.009928 Show Abstract
46. Lim A, Kumar V, Hari Dass SA, et al. Toxoplasma gondii infection enhances testicular steroidogenesis in rats. Mol Ecol. 2013;22(1):102–110. PubMed doi:10.1111/mec.12042 Show Abstract
47. Flegr J, Lindová J, Kodym P. Sex-dependent toxoplasmosis-associated differences in testosterone concentration in humans. Parasitology. 2008;135(4):427–431. PubMed doi:10.1017/S0031182007004064 Show Abstract
48. Book A, Starzyk K, Quinsy V. The relationship between testosterone and aggression: a meta-analysis. Aggress Violent Behav. 2001;6(6):579–599. doi:10.1016/S1359-1789(00)00032-X
49. Coccaro EF, Lee R, Kavoussi RJ. Aggression, suicidality, and intermittent explosive disorder: serotonergic correlates in personality disorder and healthy control subjects. Neuropsychopharmacology. 2010;35(2):435–444. PubMed doi:10.1038/npp.2009.148 Show Abstract
50. Coccaro EF, Lee R, Vezina P. Cerebrospinal fluid glutamate concentration correlates with impulsive aggression in human subjects. J Psychiatr Res. 2013;47(9):1247–1253. PubMed doi:10.1016/j.jpsychires.2013.05.001 Show Abstract
51. Ball HJ, Sanchez-Perez A, Weiser S, et al. Characterization of an indoleamine 2,3-dioxygenase-like protein found in humans and mice. Gene. 2007;396(1):203–213. PubMed doi:10.1016/j.gene.2007.04.010 Show Abstract
52. Notarangelo FM, Wilson EH, Horning KJ, et al. Evaluation of kynurenine pathway metabolism in Toxoplasma gondii-infected mice: implications for schizophrenia. Schizophr Res. 2014;152(1):261–267. PubMed Show Abstract
53. Vyas A, Kim SK, Giacomini N, et al. Behavioral changes induced by Toxoplasma infection of rodents are highly specific to aversion of cat odors. Proc Natl Acad Sci U S A. 2007;104(15):6442–6447. PubMed doi:10.1073/pnas.0608310104 Show Abstract
54. Berdoy M, Webster JP, Macdonald DW. Fatal attraction in rats infected with Toxoplasma gondii. Proc Biol Sci. 2000;267(1452):1591–1594. PubMed doi:10.1098/rspb.2000.1182 Show Abstract
55. Lafferty KD, Shaw JC. Comparing mechanisms of host manipulation across host and parasite taxa. J Exp Biol. 2013;216(pt 1):56–66. PubMed doi:10.1242/jeb.073668 Show Abstract
56. Webster JP, Kaushik M, Bristow GC, et al. Toxoplasma gondii infection, from predation to schizophrenia: can animal behaviour help us understand human behaviour? J Exp Biol. 2013;216(pt 1):99–112. PubMed doi:10.1242/jeb.074716 Show Abstract
57. Flegr J. Influence of latent Toxoplasma infection on human personality, physiology and morphology: pros and cons of the Toxoplasma-human model in studying the manipulation hypothesis. J Exp Biol. 2013;216(pt 1):127–133. PubMed doi:10.1242/jeb.073635 Show Abstract
58. Zhang Y, Träskman-Bendz L, Janelidze S, et al. Toxoplasma gondii immunoglobulin G antibodies and nonfatal suicidal self-directed violence. J Clin Psychiatry. 2012;73(8):1069–1076. PubMed doi:10.4088/JCP.11m07532 Show Abstract
59. Soyka M. Neurobiology of aggression and violence in schizophrenia. Schizophr Bull. 2011;37(5):913–920. PubMed doi:10.1093/schbul/sbr103 Show Abstract
60. Ballester J, Goldstein T, Goldstein B, et al. Is bipolar disorder specifically associated with aggression? Bipolar Disord. 2012;14(3):283–290. PubMed doi:10.1111/j.1399-5618.2012.01006.x Show Abstract
https://www.psychiatrist.com/jcp/article/Pages/2016/v77n03/v77n0313.aspx
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
【猫による被害まとめ】
1.糞尿・スプレーによる悪臭。
2.駐車中の車への傷つけ・スプレー。
3.悪戯・喧嘩による庭の破壊。
4.ペットへの加害・捕食。
5.網戸等の破壊。
6.ゴミ漁りによる散らかし。
7.蚤・トキソプラズマ等の、寄生虫・菌・ウィルスの感染媒体となり人に感染、若しくは中継。
※公園で野良猫に餌やりをされた為に野良猫が集まり、砂場が猫のトイレと化し子供達が遊べなくなるケースも発生しています。
![]()
住民「ちゃんとクソの始末もしろよ」 ※
猫狂「どんどん窮屈な世の中になった」
住民「だからちゃんとクソの始末もしろよ」
猫狂「猫嫌いはキチガイ。みんな死ねばいい」
住民「そうじゃなくてクソの始末しろよ」
猫狂「ちゃんと去勢だってしてるし地域猫はいてもいい」
住民「だからクソの始末しろよ」
猫狂「ネズミとか・・・」
住民「クソの始末のハナシしてんだよ」
猫狂「ペストとか・・・」
住民「平成の世にペストがなんだって?クソさせるなよ」
猫狂「猫嫌いは猟奇殺人予備軍」
住民「クソの始末はどうした?」
猫狂「猫嫌いは人間同士の排除までやって最後は滅びる」
住民「クソの始末は誰がやるんだよ」
猫狂「猫嫌いはモンスターペアレンツ」
住民「猫のクソの話をしてるんだよクソの」
猫狂「猫嫌いは精神病質を抱えたファシスト」
住民「そうじゃないだろクソの始末の話だよ」
猫狂「犬の鳴き声とか・・・」
住民「クソの話をしてるんだよ猫の」
猫狂「猫嫌いは自分の子供も家に閉じ込める」
住民「人間の子は他所の庭でクソしないだろ」
※くりかえし
Toxoplasma. Mind controlling parasite Must watch
A Brain Parasite Might Be Making Us Angrier
映画『スリザー』予告
-------------------------------------------------------猫様に奉仕するため社会と戦った、猫真理教の聖戦士たちを紹介します。
●2009/08/27 「猫に餌」を注意され、隣家女性を刺殺 70歳の男を逮捕
27日午後1時40分ごろ、千葉県船橋市習志野台で「包丁を持った男が女性を追いかけている」と110番通報があった。船橋東署員が現場にかけつけると、女性が自宅付近で腹部から血を流して倒れており、同署は殺人未遂の現行犯で、女性の脇に包丁を持って立っていた、近くに住む無職、林喜市容疑者(70)を逮捕した。
女性は病院に搬送されたが、間もなく死亡。同署は殺人容疑に切り替えて捜査している。
同署の調べによると、林容疑者は同日午後1時40分ごろ、隣に住む無職の女性(64)の腹部を包丁で2回刺して殺害した疑いが持たれている。
林容疑者が2年ほど前から野良猫の餌付けをしていたことを巡り、女性とトラブルになっていた。同署の調べに林容疑者は「猫のことで注意され頭にきてやった」と供述しているという。
-------------------------------------------------------
●2009/05/25 野良猫に餌をやらないよう注意されたことを逆恨み 大家刺殺に懲役22年判決
横浜地裁
川崎市のアパートで昨年6月、野良猫に餌をやらないよう注意されたことを発端に大家の男性(当時76)を刺殺、その長男の妻にもけがを負わせたとして殺人と傷害の罪に問われた同市川崎区浜町3丁目、無職高田正雄被告(70)に対する判決公判が25日、横浜地裁川崎支部であり、加登屋健治裁判長は懲役22年(求刑懲役25年)の有罪判決を言い渡した。
判決などによると、昨年6月5日午後、高田被告は前日に大家の妻から猫に餌をやらないよう注意されたことに不満を持って自室で騒ぎ、注意しに来た大家の首をナイフで刺すなどして失血死させた。さらに大家の長男の妻の顔をバールで殴って2カ月のけがを負わせた。
-------------------------------------------------------
●2007/07/27 飼い猫トラブルで隣人刺す 70歳男逮捕…大阪
飼い猫を巡るトラブルで苦情を言いに来た男性を包丁で刺し、全治2週間のけがを負わせたとして、大阪府警は26日、東大阪市、無職、中田光一容疑者(70)を殺人未遂容疑で逮捕した。
調べによると、中田容疑者は同日午後10時半ごろ、同じアパートに住む男性(54)の右胸を、自宅にあった包丁で刺した疑い。
-------------------------------------------------------
●2003/12/08 猫の仕返しと線路に石 電車妨害の男逮捕
8日午後3時10分ごろ、大阪府貝塚市のJR阪和線和泉橋本-東貝塚間で、線路に自転車の車輪や石などがあるのを白浜発新大阪行き特急「くろしお16号」の運転士が発見緊急停車した。運転士が線路脇に除き、約5分後に運転を再開。 けが人はなかった。
線路脇にいた男が投げ入れたと認め、貝塚署は往来危険の疑いで住所不定、無職藤田英久容疑者(52)を 逮捕した。「飼っていた猫が電車にはねられて死に、仕返ししようと思った」と供述したという。
調べでは、藤田容疑者は自転車の車輪2つと段ボール箱、重さ5キロの石を線路に投げ入れた疑い。
JR西日本によると、上下計2本が運休、上下計13本が最大8分遅れ、約2900人に影響した。
-------------------------------------------------------
名須川早苗(51)2014.4.30 札幌市北区警察施設や大型店で5件のガスボンベ爆発を起こし、激発物破裂の容疑で逮捕。野良猫の餌やりで周囲住民とトラブルを起こし、警察ともめていた模様(現在捜査中)。
-------------------------------------------------------
藤井ミヤ子(62)2014.4.20 大阪市阿倍野区民家に置かれていた猫よけシートに放火し、現住建造物等放火未遂の容疑で逮捕。
-------------------------------------------------------
出水衛(48)2013.12.11 大阪府和泉市飼い猫約20匹と野良猫約100匹の餌代のため、民家など32件、被害額約1920万円相当の空き巣を繰り返し、窃盗容疑などで逮捕。「猫を抱きしめているのが至福の時間」と供述。
-------------------------------------------------------
片山祐輔(30)2013.2.10 東京都江東区
遠隔操作ウィルスで他人のパソコンを乗っ取って犯罪予告をし、パソコン所有者4人の誤認逮捕を引き起こし社会を震撼させた。4人は濡れ衣だとの犯行声明をマスコミに送るなど、警察を挑発し続けたが、ウィルスのソースコード入り記録媒体を江ノ島で猫の首輪に付けたことで身元を特定され、威力業務妨害容疑で逮捕。
2006年に「のまネコ」を巡りエイベックスグループを脅迫し、懲役1年6ヶ月の実刑判決を受けるなど、猫への執着心が犯行や逮捕のきっかけとなっている。
-------------------------------------------------------
早川充益(39)2013.1.12 名古屋市西区
父経営の不動産会社に勤めていたが、「東日本大震災の原発事故で置き去りにされた動物を救う」と被災地に入り、会社が契約者から預かった数千万円の金を横領して犬猫の飼育費などに流用。
横領が発覚したため、両親と義理の祖母を絞殺し、小牧市の山中で自殺。
-------------------------------------------------------
動物愛護団体ら15人 2012.1~9月 福島県双葉市
福島県警双葉署は、福島第一原発事故の警戒区域に無許可で立ち入ったとして、災害対策基本法違反容疑で15人を摘発していたことを2012年9月24日に報告。
-------------------------------------------------------
高田光弘(74)2012.1.24 埼玉県毛呂山町
息子が飼い猫を虐めていると思い込み、口論の末首を閉めて殺害。殺人容疑で現行犯逮捕。
-------------------------------------------------------
西原康太(26)奈奈(30)2011.10.31 広島県東広島市
猫の尿や毛などが散乱した不潔な部屋に生後2ヶ月の次男を置き、皮膚炎を発症させ死亡させた。保護責任者遺棄致傷の容疑で逮捕。
-------------------------------------------------------
小坂雄造(39)里美(27)2011.5.26 千葉県柏市
長男(2)に食事を与えず餓死させ、保護責任者遺棄致死の疑いで逮捕。「子どもより猫の方がかわいかった」と供述。
-------------------------------------------------------
宍井良夫(65)2011.3.30 静岡県湖西市
野良猫に餌やりしていた公園で、市の職員と共に野良猫を駆除していた男性にカッターナイフを突きつけて脅し、暴力行為容疑で逮捕。逮捕するため自宅に訪れた警察官も殴りつけ、傷害の現行犯。
-------------------------------------------------------
坂本とし子(58)2011.3.4 千葉県勝浦市
猫の飼育方法を指導しに来た保健所職員の顔をひっかいたとして、公務執行妨害と傷害容疑で現行犯逮捕。
-------------------------------------------------------
佐々木祐一(65)2010.11.13 埼玉県寄居町
猫同士の喧嘩が元で相手の飼い主の頭や顔を木刀で殴り、重傷を負わせた。殺人未遂容疑で逮捕。
-------------------------------------------------------
水元努(31)2010.9.1 北海道留萌市
「ペットの猫が死んでむなしくなった」と高速道路を約100km逆走し、道路交通法違反の疑いで現行犯逮捕。
-------------------------------------------------------
会社役員の女(48)2010.4.27 岐阜市
米国に残したペットの猫に会うため、偽造パスポートで米国へ渡航を繰り返したとして、旅券法違反の罪で懲役1年6カ月の判決。
-------------------------------------------------------
板橋静男(72)2010.4.24 埼玉県川口市
団地で猫を追いかけていた男児(9)のあごを締め上げるなどし、暴行容疑で逮捕。
段ボールで野良猫の家を作り餌を与えるなど、団地内で有名。
-------------------------------------------------------
林喜市(70)2009.8.27 千葉県船橋市
女性から野良猫の餌やりを注意され、その帰宅を待ち伏せして包丁で刺殺。殺人罪で懲役17年の判決。
-------------------------------------------------------
平野幸男(73)2008.10.22 長崎市
犬の散歩に通りかかった男性を、餌やり中の野良猫が逃げたからと木刀で脅し、暴力行為容疑で逮捕。
-------------------------------------------------------
永吉教幸(72)2008.7.5 栃木県小山市(ホームレス)
寝泊まりしている公園で野良猫を抱いた人を、猫を虐めていると勘違いし鉄パイプで殴り、現行犯逮捕。
-------------------------------------------------------
20歳の夫婦 2008.7.3 福岡市
生後1ヶ月の乳児に食事を与えず、育児放棄で虐待死させる。保護責任者遺棄致死容疑で逮捕。
乳児は猫のトイレにしていた段ボールに寝かせていた。「子供より猫の方が可愛かった」と供述。
-------------------------------------------------------
河田教晴(28)2008.6.19 大阪市
無職・生活保護受給者で猫5匹飼う。餌代に困り何度もコンビニに押し入り、強盗容疑で逮捕。
-------------------------------------------------------
高田正雄(69)2008.6.5 神奈川県川崎市
アパートの大家に餌やりを注意されて逆上し、サバイバルナイフで大家を刺殺、大家の義理の娘にも重傷を負わせ、殺人及び傷害罪で懲役22年の判決。
-------------------------------------------------------
中田光一(70)2007.7.27 大阪市
猫被害の苦情を言いに来たアパートの隣人を包丁で刺し、殺人未遂容疑で逮捕。
-------------------------------------------------------
静岡県伊東市の老人(81)2006.8.24
ペット禁止の市営住宅で猫を放し飼いしていることを市に告げ口されたと妄想、上の階に住む姉妹に言い掛かりを付けた挙げ句にノコギリで殴り、傷害容疑で逮捕。
-------------------------------------------------------
中島数男(73)2005.4.24 兵庫県尼崎市
猫の餌付けに苦情を言った人の部屋へ包丁を持って押し込み乱闘に。暴力行為(脅迫)容疑で逮捕。
-------------------------------------------------------
荒木正道(60)2005.8.29 埼玉県吹上町
猫糞で迷惑していた隣人を金属バットで小突くなどして、傷害容疑で逮捕。
-------------------------------------------------------
藤田英久(52)2003.12.8 大阪府貝塚市
電車に轢かれた猫の仕返しに、線路に自転車のタイヤや段ボール、石などを置き、往来危険容疑で逮捕。
----------------------------------------------------------------
古美術商殺人事件 容疑者宅に放置された21匹のネコを保護(餌やり猫愛誤の子供は殺人鬼に育つ)(トキソプラズマ)(弓形蟲感染症)
https://www.news-postseven.com/archives/20140606_259567.html
東京・国立市の古美術商強殺事件 被告の無期懲役が確定(餌やり猫愛誤の子供は殺人鬼に育つ)(トキソプラズマ)(弓形蟲感染症)②
https://www.sankei.com/affairs/news/151017/afr1510170018-n1.html
東京・国立市の古美術商強盗殺人で男に無期懲役の判決(餌やり猫愛誤の子供は殺人鬼に育つ)(トキソプラズマ)(弓形蟲感染症)③
http://jwssnnews.blog.jp/archives/43572982.html
----------------------------------------------------------------
戦後最大の大量殺人鬼・植松聖容疑者の全貌(餌やり猫愛誤の子供は殺人鬼に育つ)(トキソプラズマ)(弓形蟲感染症)
https://matome.naver.jp/odai/2146960319854545001?&page=1
植松聖容疑者 犯行直前の美容整形手術費用は80万円
https://www.news-postseven.com/archives/20160803_435837.html?PAGE=2
----------------------------------------------------------------
弟を「練炭殺害」した姉の実父も怪死 自身のブログでは動物殺処分への怒り綴る(餌やり猫愛誤の子供は殺人鬼に育つ)(弓形蟲感染症)
https://dot.asahi.com/dot/2018070100014.html?page=1
https://headlines.yahoo.co.jp/article?a=20180701-00000014-sasahi-soci
練炭自殺装い弟殺害 44歳の姉に離婚トラブルで元夫の定期に大麻入れた過去
https://dot.asahi.com/wa/2018062400003.html?page=1
弟を殺害で起訴 朱美被告が綴った「練炭殺人日記」全文入手
https://dot.asahi.com/wa/2018071100098.html?page=1
----------------------------------------------------------------
会うと会釈、「人当たりいい子」 警官刺殺容疑の大学生(餌やり猫愛誤の子供は殺人鬼に育つ)(トキソプラズマ)(弓形蟲感染症)
https://www.asahi.com/articles/ASL9M6K55L9MUTIL06F.html?iref=pc_ss_date
仙台・警官刺殺・容疑の大学生に「礼儀正しい子なぜ」(餌やり猫愛誤の子供は殺人鬼に育つ)(トキソプラズマ)(弓形蟲感染症)②
https://mainichi.jp/articles/20180920/k00/00m/040/156000c
仙台・交番襲撃の大学生 包丁以外にも多くの凶器持つ(餌やり猫愛誤の子供は殺人鬼に育つ)(トキソプラズマ)(弓形蟲感染症)③
https://www.oricon.co.jp/article/560069/
警官刺殺容疑者「おとなしくて礼儀正しかった」
https://headlines.yahoo.co.jp/hl?a=20180920-00050040-yom-soci
-----------------------------------------------------------
脳をあやつる虫(トキソプラズマ)(弓形蟲感染症)(狂犬病)
http://www.nikkei-science.com/page/magazine/0306/parasite.html
トキソプラズマが人の脳を操る仕組み
http://natgeo.nikkeibp.co.jp/nng/article/news/14/7449/-----------------------------------------------------------------------------
起業したい人は猫のウ●コ食べればできるかも!(良い子は真似しないように、危険です)-----------------------------------------------------------------------------
-------------------------------------------------------
猫オタのロリコン勝又拓哉が2005年栃木県今市市で下校途中の7歳の女児を車で拉致して
わいせつ行為をしたあとに胸をメッタ刺しにして殺害して雑木林に遺棄した残虐な事件
勝又拓哉の飼っていた希少種の猫の毛が女児の遺体の付着していたことが逮捕の決め手
-------------------------------------------------------
ト キ ソ プ ラ ズ マ と 母 子 感 染(トキソプラズマ.弓形蟲感染症)-------------------------------------------------------
猫オタが起こした猟奇殺人事件「神戸小1女児バラバラ殺害事件」 猫オタのロリコン君野康弘が2014.年に神戸市長田区で6歳の女児を家に連れ込んで 殺害してわいせつ行為をした後に遺体をバラバラにしてビニール袋に入れて遺棄した残虐な事件 君野康弘は飼ってる猫を餌に猫好き女児を家に連れ込んでいた 勝又被告、控訴審も有罪 今市事件で東京高裁 -------------------------------------------------------
2005年12月、日光市(旧今市市)大沢小1年だった吉田有希ちゃん=当時(7)=が殺害された 今市事件で、殺人罪に問われた鹿沼市西沢町、無職勝又拓哉被告(36)の控訴審判決公判が 3日午前、東京高裁で開かれた。藤井敏明裁判長は、無期懲役を言い渡した一審宇都宮地裁の 裁判員裁判判決を破棄したが、被告に無期懲役を言い渡した。 https://headlines.yahoo.co.jp/hl?a=20180803-03057321-soon-l09
-----------------------------------------------------------------------
狂犬病どんな病気か?(狂犬病)
狂犬病~もし咬まれたら,すぐに医療機関へ(狂犬病)
犬・猫回虫症(イヌ回虫.犬蛔蟲.Toxocara canis)(猫回虫.貓蛔蟲.Toxocara cati)⑥
回虫症(イヌ回虫.犬蛔蟲.Toxocara canis)(猫回虫.貓蛔蟲.Toxocara cati)⑦
消化管内の寄生虫(イヌ回虫.犬蛔蟲.Toxocara canis)(猫回虫.貓蛔蟲.Toxocara cati)⑧
イヌ・ネコ回虫感染症(イヌ回虫.犬蛔蟲.Toxocara canis)(猫回虫.貓蛔蟲.Toxocara cati)⑨
成人肺トキソカラ症8例(イヌ回虫.犬蛔蟲.Toxocara canis)(猫回虫.貓蛔蟲.Toxocara cati)⑩
 創作內容
創作內容
 人と動物の共通感染症 (165)
人と動物の共通感染症 (165)