病因學Etiology
病因學Etiology◆ 過敏和氣喘之病因有著密切的關係,結合了基因和環境因素,經由複雜細胞激素之交叉作用決定了過敏和氣喘之易感受性(susceptibility)。環境當中會促發氣喘病的因子有病毒、過敏原和職業上之暴露於某些刺激物。異位過敏體質亦是受基因控制而容易對於環境中過敏原產生大量免疫球蛋白E(IgE)之反應,它是氣喘發病原因中可找出最明確的誘發因子。
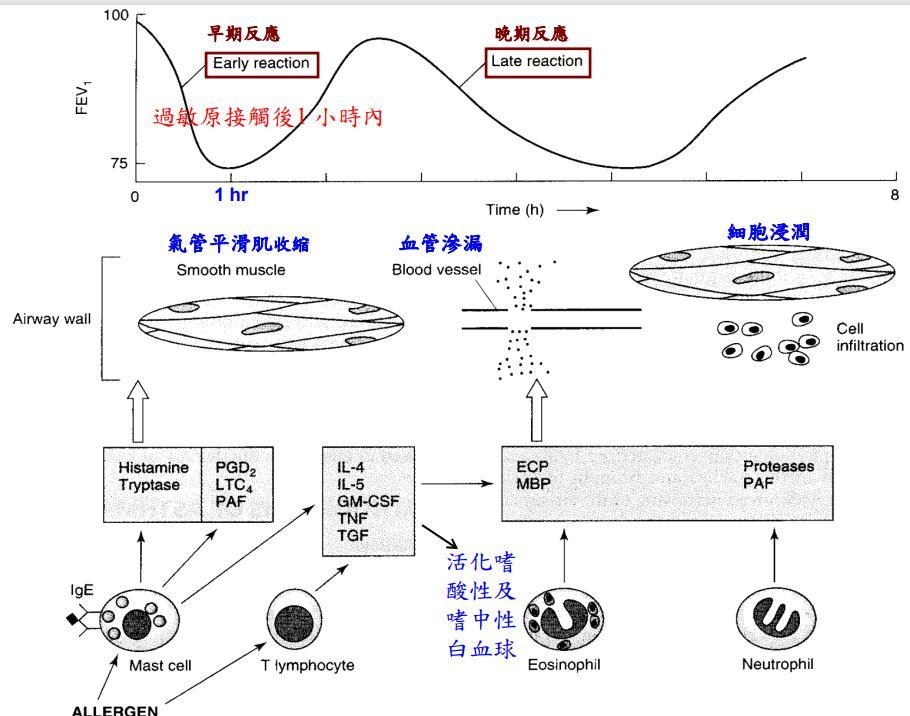
◆ 特異性IgE 和肥大細胞及嗜鹼性細胞上之高親和性接受器( FcεRI ) 結合稱為致敏現象(sensitization)。氣喘病人已致敏的肥大細胞和過敏原所引起的反應區分為早期氣喘反應(Early phase asthmatic response, EAR) 和晚期氣喘反應(Late phase asthmatic response, LAR)
◆早期氣喘反應會使肥大細胞釋放出組織胺和其他已形成之介質。在和過敏原接觸後1 小時內會造成短暫之第1 秒用力呼氣容積 (forced expiratory volume in 1 second, FEV1)下降,然後在接觸過敏原2~8小時內會接著出現晚期氣喘反應,此時氣道會有多種發炎細胞浸潤,同時出現為期較長且較嚴重之氣道阻塞。連續長期接觸過敏原引起之持續性晚期氣喘反應即造成了慢性氣道之症狀,包括長期咳嗽、胸悶、呼吸不順暢、喘鳴 。 IgE 抗體具有能被動傳遞早期氣喘反應和晚期氣喘反應敏感性之能力,這種IgE 介入之肥大細胞活化作用引起了慢性組織嗜酸性白血球浸潤和氣道壁變型,這代表氣道結構上不可逆之變化和長期肺功能之惡化
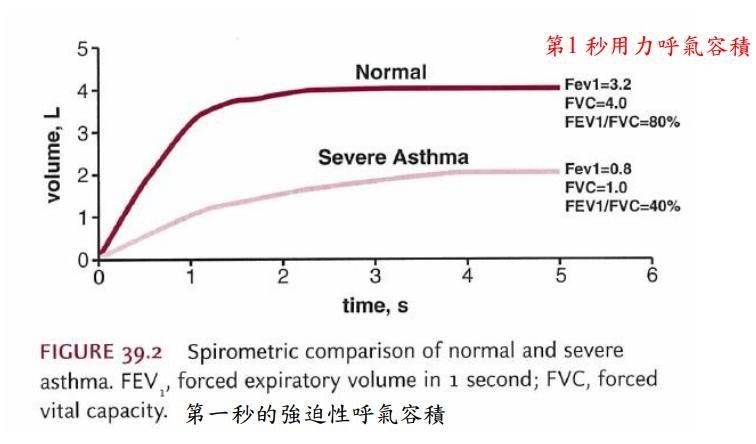
FVC 是指盡最大吸氣後,盡力呼氣所能呼出的最大氣量。
◆ FVC 是測定呼吸道有無阻力的重要指標。常用第 1 秒肺活量( FEV1 )占整個肺活量百分比表示,稱 1 秒率 (FEV1/FVC) 正常值應 >80%
<80% 提示氣道阻塞性通氣障礙,如 COPD 、Asthma 急性發作時,FEV1 及 FEV1/FVC 皆 下降。
病理學◤早期氣喘發作機制:
◆通常是由於IgE調控失當所引起 > on re-exposure to an antigen, antigenantibody interaction on the surface of the mast cells triggers both the release ofmediators stored in the cells‘ granules and the synthesis and release of other mediators > responsible for the immediate bronchoconstriction (立即性的支氣管收縮 )and vascular leakage (血管滲漏)
◤晚期氣喘發作機制:
◆ Other mediators are responsible for the more sustained bronchoconstriction (持續性的支氣管收縮), cellular infiltration (細胞浸潤 )of the airway mucosa, and mucus hypersecretion (黏液過度分泌) of the late asthmatic reaction (後期的氣喘反應) that occurs 2-8 hours later > these mediators are thought to be cytokines (細胞激素)
characteristically produced by TH2 lymphocytes
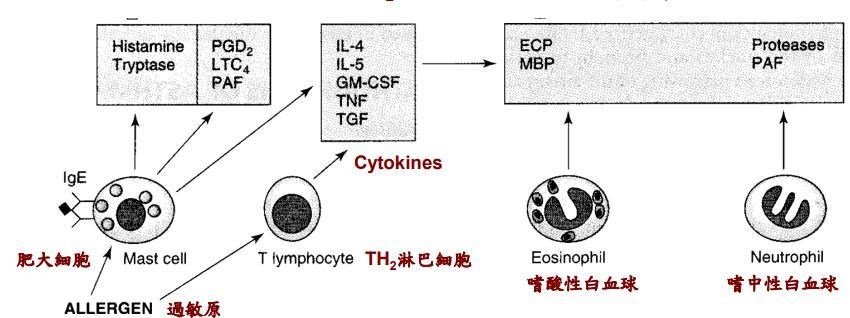
◆ Exposure to allergen (曝露於過敏原中導致IgE活化, 與'吸道黏膜的肥大細胞結合
◆ On re-exposure to allergen, antigen-antibody interaction on mast cell surfaces triggers release of mediators of anaphylaxis 影響氣喘的過敏反應介質: histamine組織胺, tryptase, prostaglandin D2前列腺素, leukotriene C4白三烯素, and platelet-activating factor (PAF)血小板啟動因子
◆氣管立即收縮導致 the immediate fall in FEV1 (第一秒鐘的強迫性呼氣容積立即性下降)
◆Re-exposure to allergen also causes the synthesis and release of a variety of cytokines
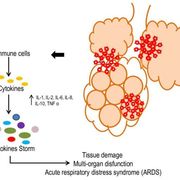
(再次暴露於過敏原時同時也造成許多細胞激素的合成與釋放): interleukins 4 and 5, granulocyte-macrophage colony stimulating factor (GM-CSF), tumor necrosis factor (TNF), and tissue growth factor (TGF) from T cells and mast cells
◆These cytokines in turn attract and activate eosinophils and neutrophils (這些細胞激素會活化嗜酸性及嗜中性白血球), whose products include eosinophil cationic protein (ECP), major basic protein (MBP), proteases, and platelet-activating factor
◆ These mediators cause the edema (水腫), mucus hypersecretion (黏液過度分泌), smooth muscle contraction (平滑肌收縮), and increase in bronchial reactivity (支氣管反應性增加) associated with the late asthmatic response, indicated by a fall in FEV1 2-8 hours after the exposure (暴露過敏原2-8小時後FEV1下降為後期的氣喘反應)
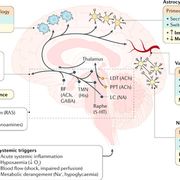
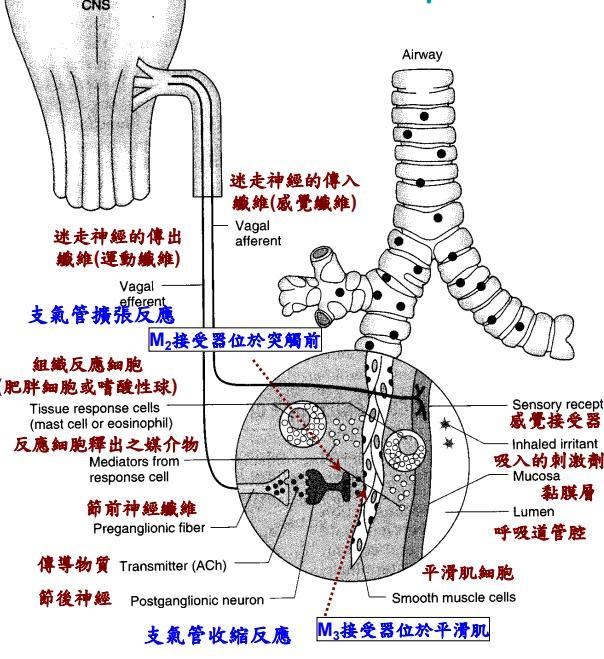
◆迷走神經中的傳入通路到達 CNS,從 CNS 的傳出通路到達傳出神經節 > 節後纖維釋放乙醯膽鹼 (Ach),它與氣道平滑肌上的毒蕈鹼受體結合 •>吸入的物質可能通過幾種可能的機制引起支氣管收縮 – 首先,它們可能會觸發肥大細胞中化學介質的釋放 – 其次,它們可能會刺激傳入受體以啟動反射性支氣管收縮或釋放直接刺激平滑肌收縮的速激肽(例如sustance P P 物質)。
 治療目標與預防
治療目標與預防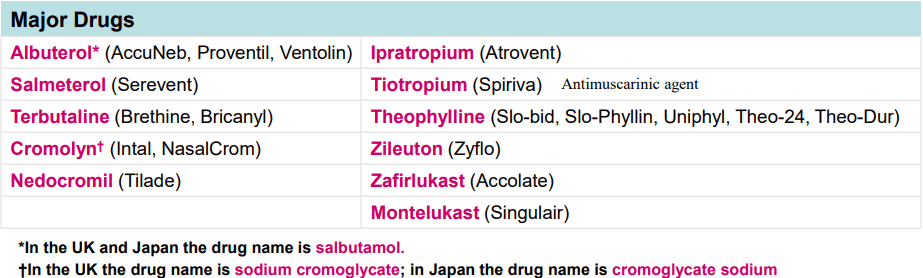
◆1.減少肥大細胞結合IgE的量抗IgE抗體
2.防止肥大細胞去顆粒化(預防肥大細胞去顆粒化)>cromolyn or nedocromil, sympathomimetic agents, calcium channel
3.阻斷化學傳導介質釋放> antihistamines and leukotriene receptor antagonists
4. Inhibit the effect of acetylcholine released from vagal motor nerves (抑制從迷走神經所釋放的Ach之作用)> muscarinic antagonists
5. Directly relax airway smooth muscle (直接鬆弛呼吸道平滑肌) >sympathomimetic agents, theophylline
◆茶鹼不僅可以逆轉或預防,還可以降低支氣管反應強度,但是初始服用會引發一些思考及知覺方面的困難。在早期的時候會先呈現出一些注意力、記憶力功能方面的障礙。
★治療總綱
THERAPEUTIC OVERVIEW
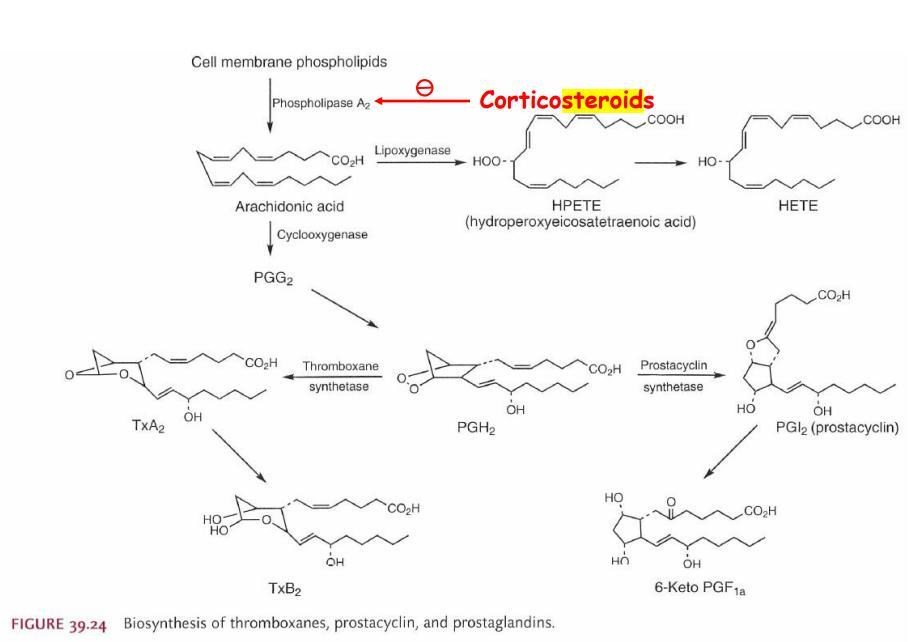
Antiinflammatory agents
• Chromones for controlling mediator release from mast and other cells and for their generalized membranestabilizing effects 。具有細胞膜穩定作用進而抑制發炎介質的釋放
• Glucocorticoids, local or systemic, for controlling transcription of mediator genes, and for controlling edema,mucus production, and eosinophil infiltration 。抑制發炎介質基因的轉錄,降低水腫、黏液產生及細胞浸潤
• Leukotriene modulators to decrease inflammatory mediator synthesis or antagonize inflammatory mediatorreceptors。 降低發炎介質的合成或拮抗其接受器
Bronchodilators
• Methylxanthines for reducing the frequency of recurrent bronchospasm 減少復發性支氣管痙攣發生的頻率
• β2-Adrenergic receptor agonists for relaxing bronchial smooth muscle and decreasing microvascular
permeability 鬆弛支氣管平滑與降低微血管滲透性
• Muscarinic receptor antagonists for inhibiting the bronchoconstrictor effects of endogenous acetylcholine 抑制乙醯膽鹼引起的支氣管收縮
治療(一)長期控制藥物
目的在減輕呼吸道發炎與腫脹並預防氣喘發作,必須長期每日使用。若是初期使用,可能需要數週才能出現顯著的療效。
臨床上◎常見之藥物如下:
⬜吸入型類固醇(ICS, inhaled corticosteroids):
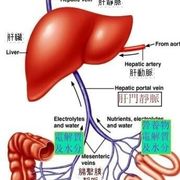
局部使用,直接作用在呼吸道; 吸入型類固醇每一下的劑量只有口服型類固醇的1/100-1/20;且經由肝臟首渡效應(first pass effects)代謝,經口吸收比例低,一般認為是治療持續性氣喘最有效的抗發炎藥物。ICS可緩解
症狀、提升肺功能、改善生活品質、減少惡化的發生、並降低因氣喘導致住院或死亡的風險。一些研究顯示:以ciclesonide、budesonide和fluticasone的全身性副作較少,因此常被用做吸入型類固醇之藥物選擇。
成人若每日使用低劑量budesonide 400 mcg或相等強度之其他藥物,治療一週後,預計可達到最大效果,且不會造成全身性影響。
◎藥理機制:
Corticosteroids have been used to treat asthma since 1950 and are presumed to act by their broad anti-inflammatory efficacy (廣泛消炎作用), mediated in part by inhibition of production of inflammatory cytokines (經由抑制發炎性細胞激素產生)。
◆They do not relax airway smooth muscle directly (不能直接鬆弛呼吸道平滑肌) but reduce bronchial reactivity (但可以減少支氣管的反應性) and reduce the frequency of asthma exacerbations (減少氣喘惡化的頻率) if taken regularly 。
◆ Because of severe adverse effects when given chronically, oral and parenteral corticosteroids are reserved for patients who require urgent treatment。
因為長期口服給予或注射類固醇會有嚴重的副作用,因此保留在緊急時治療使用。
◆For prevention of nocturnal asthma (預防夜間氣喘發作), however, oral or inhaledcorticoids are more effective when given in the late afternoon 下午。
◆ Aerosol treatment is the most effective way to decrease the systemic adverseeffects of corticosteroid therapy (噴霧劑治療是降低類固醇治療產生全身性副作用最有效的方法。)
◆副作用: A special problem caused by inhaled topical corticosteroids is the occurrence of oropharyngeal candidiasis (口咽念珠球菌炎) & hoarseness (聲音沙啞) 。
This risk can be reduced by having patients gargle water and spit after each inhaled treatment 。
◆A novel approach to minimizing the risk of toxicity from systemic absorption of an inhaled corticosteroid is the development of ciclesonide this recently approved corticosteroid is inhaled as a prodrug activated by cleavage by esterases in bronchial epithelial cells (ciclesonide為一前驅藥,由支氣管上皮細胞的酯酶活化裂解。)
◆ minimizing its risk (減少副作用的發生) of causing cutaneous thining (表皮變薄),cataracts (白內障), osteoporosis (骨質疏鬆), or temporary slowing of growing (暫時性生長變慢)。
◆但是 In contrast to b-stimulant agents and theophylline, chronic use of inhaled corticosteroids reduces bronchial reactivity (長期使用可減少支氣管的反應性 )。
◆ they are not curative (不能治癒) and are effectively only so long as they are taken (只有長期使用才有效) as “controller” 控制者。
⬜常見藥物:
Alvesco ® (Ciclesonide)
Duasma ®MDI (Budesonide)
Flixotide® (Fluticasone propionate)
Pulmicort ® Turbuhalar(Budesonide)
◆藥物化學架構
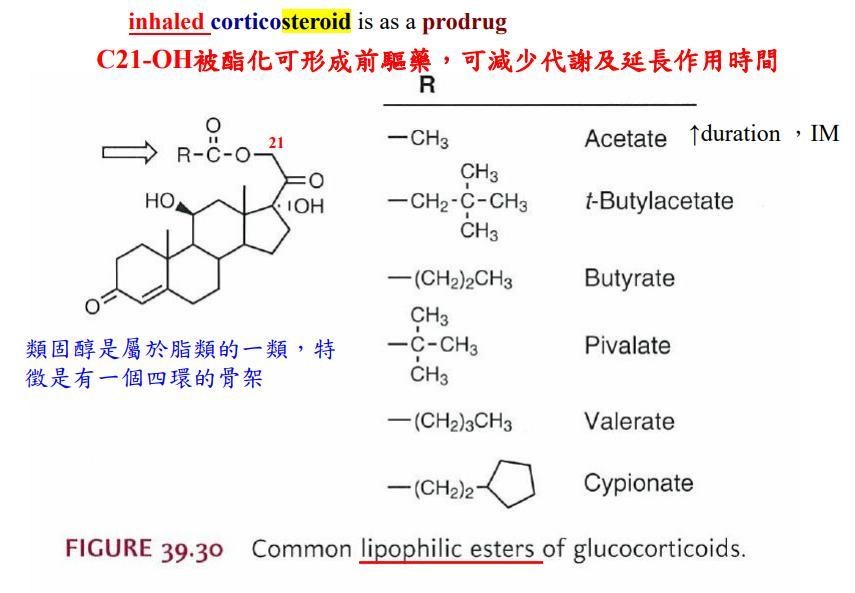
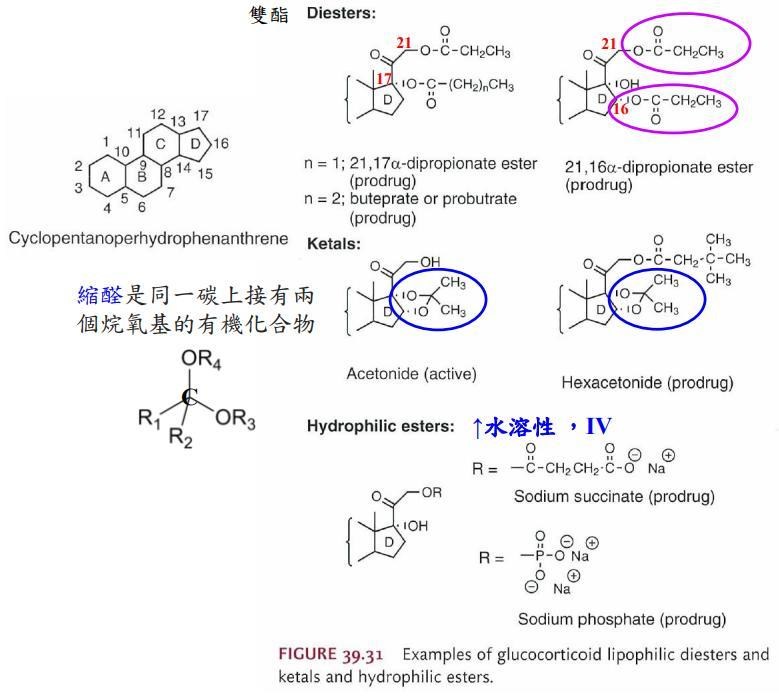
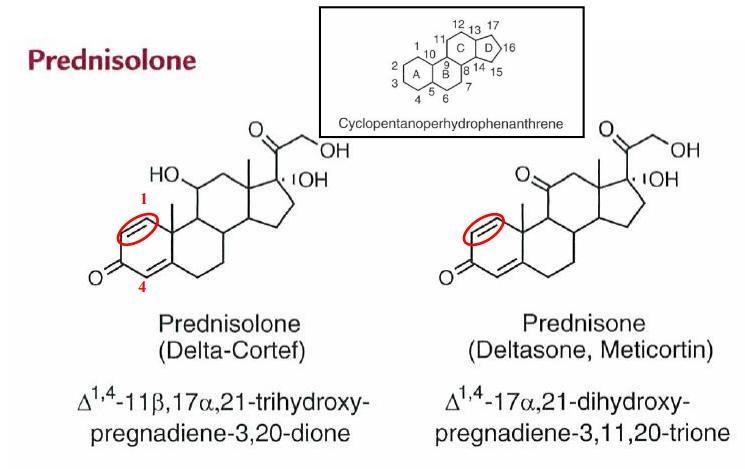
作用機制:類固醇與receptor結合後,因為結構改變 (conformational change),因此可以進入細胞核內,並結合到DNA序列上特定的荷爾蒙結合區域 (hormone response element, HRE) 影響基因的轉錄及蛋白質的合成。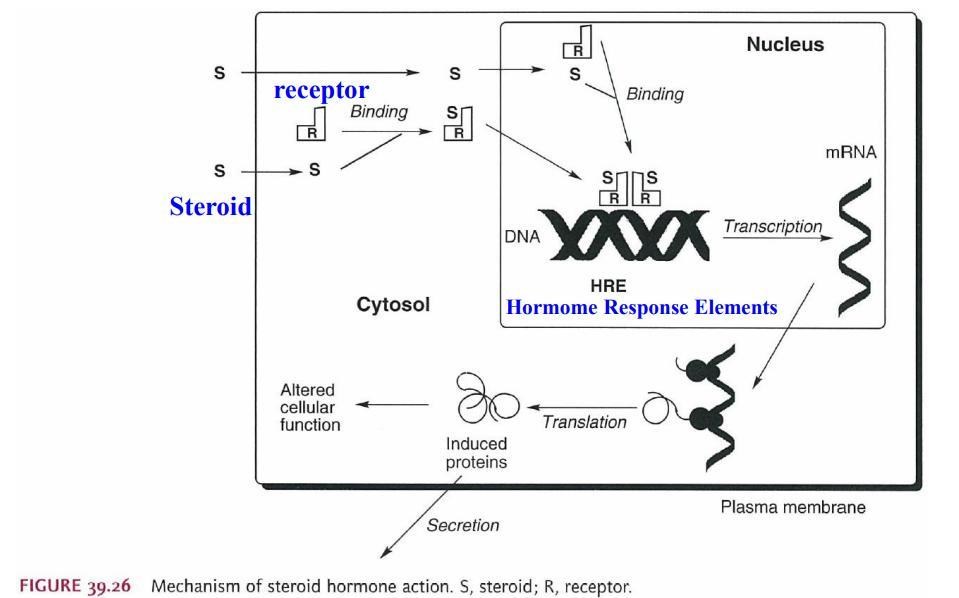
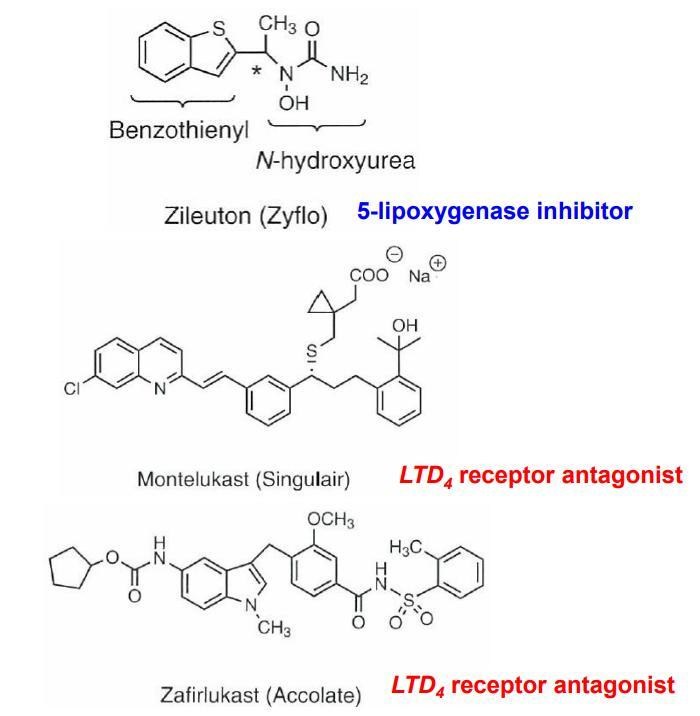
⬜白三烯(leukotriene)受體拮抗劑:
副作用少;然而,療效於成人稍不佳於ICS,但就兒童而言並無明顯差異。
常見藥物: Singulair® (Montelukast)。機制:zafirlukast and montelukast 為selective and active leukotriene receptor antagonist. It binds to cysteinyl leukotrienes type-1receptors (CysLTR1) in human airway (smooth muscle cells and macrophages), which prevent sairway edema, smooth muscle contraction and other respiratory inflammation.
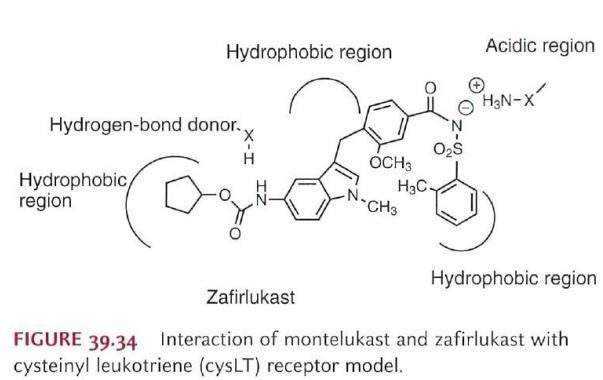
LTC4、LTD4和LTE4均含有cysteinyl殘基,又統稱為cysteinylleukotriene(CysLT),作用於其標的組織的接受器上,引起支氣管的高度反應性和慢性發炎。其接受器分為CysLTR1和CysLTR2人體氣管(平滑肌細胞和巨噬細胞)中,阻止呼吸道水腫、平滑肌收縮和其他呼吸道發炎作用。
⬜長效乙二型交感神經作用劑(Long-acting beta-2 agonists :LABA)合併吸入型類固醇(LABA-ICS):
研究顯示,長期單獨使用LABA可能會增加嚴重氣喘發作的危險性,導致住院或死亡;且LABA具有減少類固醇用量的效果 (steroid– sparingeffect)。因此,LABA需與吸入型類固醇藥物(ICS)合併使用,作為長期控制藥物。
LABA藥效可達12小時;salmeterol作用(onset)較慢,只用於長期控制藥物;而formoterol作用快速,也可同時作為緩解藥物。
◎常見藥物:
Symbicort ® (Budesonide/Formoterol)、Seretide ® (Fluticasone/Salmeterol)、
Foster® (Beclomethasone/Formoterol) 。
◎藥物化學架構:
◎長效抗膽鹼藥物(long-acting muscarinic antagonists: LAMA):
之前只用於 COPD (chronic obstructive pulmonary disease 慢性阻塞性肺病)的藥物,在經歷臨床試驗研究後已取得治療氣喘的適應症,但屬於後線藥物,即GINA step4/5。美國 FDA於 2015年九月核准,台灣 TFDA也核准了,適應症增加"適用於已接受吸入性皮質類固醇 (每日劑量相當於≥800 μg Budesonide)與長效 β2促進劑而仍未控制症狀,且過去一年發生一次或以上嚴重惡化之成人支氣管氣喘患者,作為維持性支氣管擴張劑附加治療。
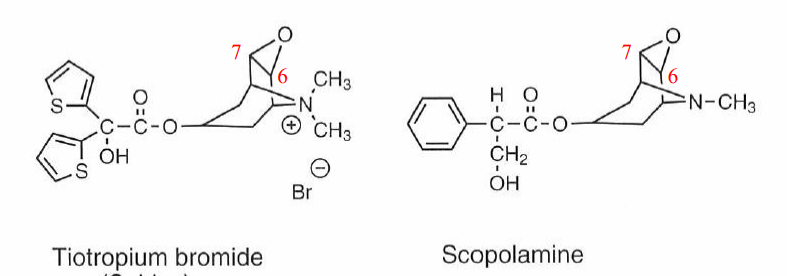
⬜常見藥物:Spiriva® (Tiotropium)。
⬜藥理機轉/藥物化學結構分析
1. 抑制氣管平滑肌上的M3接受體,會使氣管放鬆。此乃競爭性與可逆的拮抗作用。
2. 作用可持續長達24小時以上。長效作用可能是因為tiotropium與M3接受體的分離速度很慢,其分離半
衰期很明顯地長於ipratropium。
3. Tiotropium為4級胺之抗膽鹼性劑,當吸入時,可局部選擇性作用於支氣管,在產生有效治療濃度時
也不會產生全身性抗膽鹼作用。
4. 在體外功能性試驗中,tiotropium與M2接受體分離的速度較M3快,因此以動力學的角度而言,對M3接
受體的選擇性高於M2。
5. 與接受體作用強且分離速度慢,所以在臨床上治療慢性阻塞性肺疾 (COPD) 之患者有顯著且長效的支
氣管擴張作用。
◎緩釋型茶鹼:藥效比上述類固醇及白三烯調節劑弱,且治療範圍狹窄,屬於後線用藥;但由於藥效長,約12小時,多用作夜間發作之輔助治療。
◎常見藥物:
Phyllocontin ® (aminophylline), Xanthium ® (theophylline)。
◎藥化結構與機制:
Theophylline在緩解性氣喘比交感神經用藥療效更強且便宜
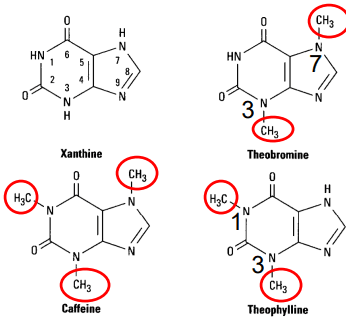
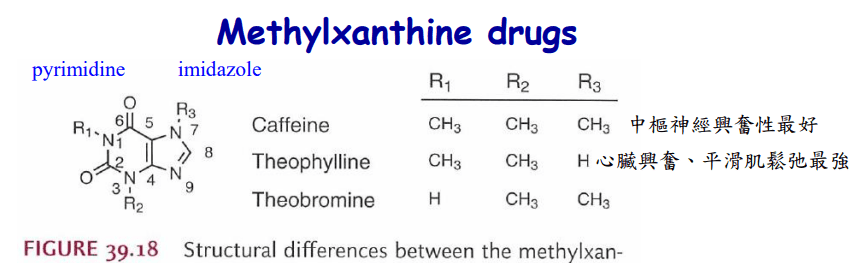
Theophylline 1,3-dimethylxanthine;
theobromine 結構屬於 3,7-dimethylxanthine;
caffeine 結構屬於1,3,7-trimethylxanthine (脂溶性最高)
每人每日咖啡因攝取若超過250毫克(約2~3杯咖啡)會產生焦躁感、興奮、睡眠障礙、噁心、頻尿、脈搏加速等症狀
每人每日咖啡因攝取若超過250毫克(約2~3杯咖啡)會產生焦躁感、興奮、睡眠障礙、噁心、頻尿、脈搏加速等症狀
◎Theophylline直接產生氣管擴張效應與抑制發炎反應,在高劑量情形下,還可以 inhibit several members of the phosphodiesterase (PDE) enzyme family (抑制多種PDE的異構酶) & another proposed mechanism is the inhibition of cell surfacereceptors for adenosine (也抑制adenosine在細胞表面的接受器)
更有藥理機制the immune and inflammatory activity of specific cells (減少特定細胞的免疫及發炎活性)
◎副作用:
nervousness (神經質) and tremor (震顫) ,促進心臟收縮增加心跳,narrow therapeutic window (治療指數很窄),因此冠心症相關患者不建議使用
{機轉:inhibition of presynaptic adenosine receptors( 抑制突觸前adenosine接受器而增加兒茶酚胺的釋放) & calcium influx may be increased directly through the increase in cAMP that results from inhibition of phosphodiesterase 抑制PDE而增加cAMP也會增加鈣離子的流入}
nervousness (神經質) and tremor (震顫) ,促進心臟收縮增加心跳,narrow therapeutic window (治療指數很窄),因此冠心症相關患者不建議使用
{機轉:inhibition of presynaptic adenosine receptors( 抑制突觸前adenosine接受器而增加兒茶酚胺的釋放) & calcium influx may be increased directly through the increase in cAMP that results from inhibition of phosphodiesterase 抑制PDE而增加cAMP也會增加鈣離子的流入}
(二)急性期緩解藥物(reliever):只在急性發作期使用。
◎全身性類固醇:
短期使用於急性發作或是難以控制的氣喘,可以口服或是注射
◎常用藥物:hydrocortisone, prednisone, methylprednidsolone, dexamethasone。
口服使用藥物使用每日prednisone 1mg/kg qd,5-7天。注射藥物則使用
hydrocortisone 100-200 mg q6-8h。
◎短效乙二型交感神經作用劑(Short-acting beta-2 agonists :SABA):能快速且高效地緩解氣喘症狀。
Epinephrine is an effective, rapidly acting bronchodilator when injected subcutaneously (皮下) or inhaled (吸入) as a microaerosol (噴霧) from a pressurized canister
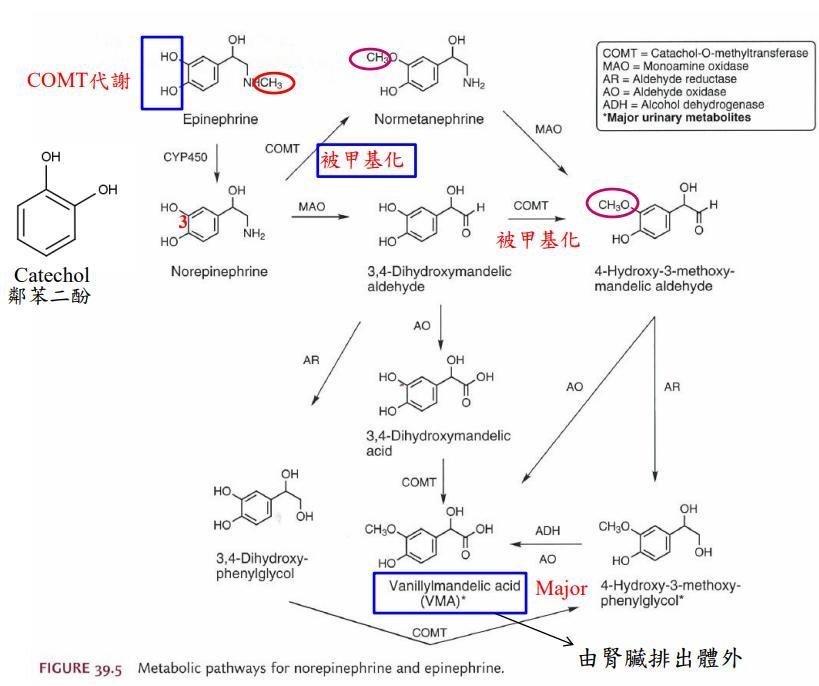
◆Because epinephrine stimulates b1 as well as b2receptors, tachycardia心搏過速, arrhythmias心律不整,and worsening (惡化) of angina (心絞痛) are troublesome adverse effects
◆Ephedrine has a longer duration, oral activity, more pronounced central effects (較強的中樞作用), and much lower potency > it is now used infrequently in treating asthma
◆ Isoproterenol, stimulates b1 as well as b2receptors, is a potent bronchodilator cardiac arrhythmias
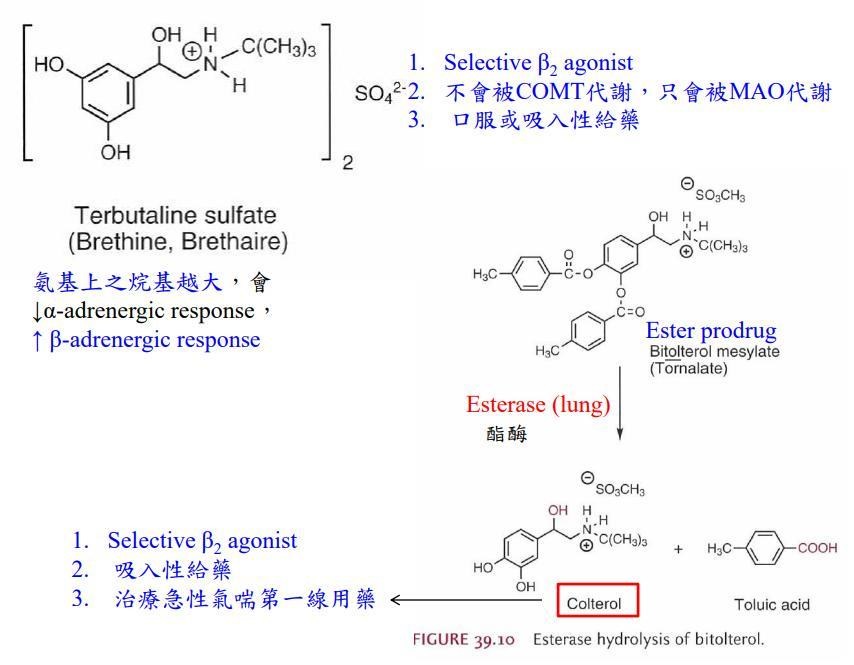
◆ The b2-selective adrenoceptor agonist drugs are the most widely used sympathomimetics (擬交感神經作用劑) for the treatment of asthma at the present time > they have a larger substitution on the amino group and in the position of the hydroxyl groups on the aromatic ring (在胺基及芳香環的-OH上有較大的取代基)
◆ Albuterol, terbutaline, metaproterenol, and pirbuterol are available as metered dose inhalers & albuterol and terbutaline are also prepared in tablet form & only terbutaline is available for subcutaneous injection(Albuterol, terbutaline, metaproterenol, pirbuterol 可作為吸入劑劑型;Albuterol與terbutaline另外可用錠劑劑型設計)
◆藥物化學架構
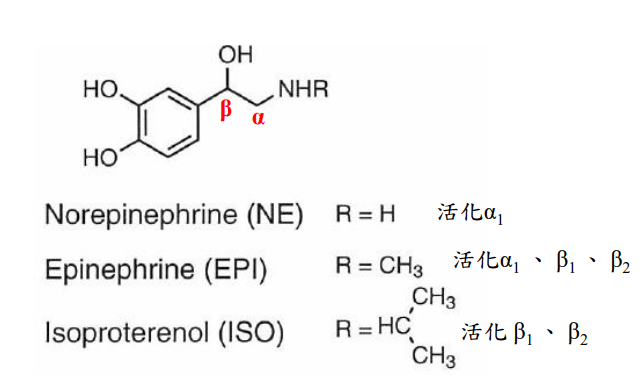
I.phenyl (苯基) 與氨基之間為2個碳原子 (α、β) 時作用最好
II. 氨基上之烷基 (R) 越大,會降低 α-adrenergic response,增加 β-adrenergic response
N接的基團R'=C2,Stimulate b1,b2
R'=C3,Stimulate b1,2,3
R'=C4 Selective Stimulate b2
R'=C5 or up Stimulate b2
III. 氨基如烷化形成3級胺,藥理活性會降低
IV.β碳上有OH取代,則具有β-adrenergic effect

◎計量吸入器
◆常見藥物:Berotec ® (Fenoterol), Ventolin® (Salbutamol), Bricanyl ® (Terbutaline)。
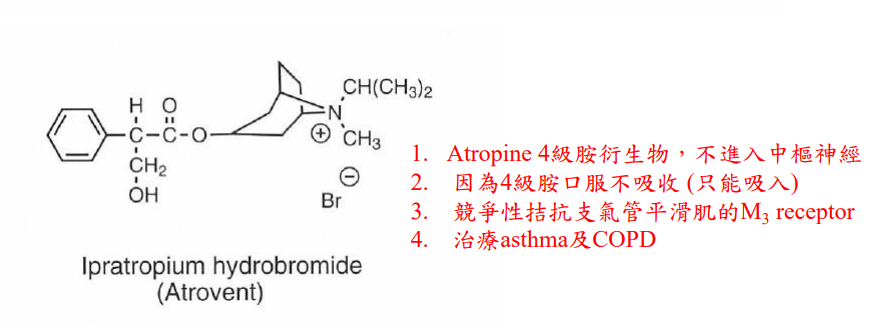
◎短效抗膽鹼藥物:(Short-acting muscarinic antagonists: SAMA):
可反轉乙醯膽鹼引起的支氣管痙攣,多為四級胺的衍生物,可在呼吸道微量吸收,且不通過血腦屏障(blood–brain barrier ,BBB),可產生較長的局部作用block the contraction of airway smooth muscle and the increase in secretion of mucus (阻斷平滑肌收縮及粘液的分泌)以吸入方式給予atropine或是atropine四級胺的衍生物可使其作用更具選擇性,作用在支氣管而非全身。
◎常見藥物:Atrovent ® (ipratropium)。
◎臨床上,SAMA在中重度氣喘患者發作時,可與SABA並用,兩者併用具有加乘作用,也可延長作用時間,比起單獨使用SAMA有較低的住院率及提高FEV1。◎常見藥物:Combivent ® (Salbutamol + Ipratropium), Berodual® (Fenoterol+ Ipratropium)
★2019 GINA新增建議以Low dose ICS-formoterol作為急性期發作(step1-5)之首選緩解藥物。
◎常見藥物:Symbicort ® (Budesonide/Formoterol) ,Foster®(Beclomethasone/Formoterol)
治療新面向氣喘病人大多是嗜酸性白血球(eosinophil)及抗免疫球蛋白 E(IgE)表現過多。
因此,目前已核准上市的藥物多以降低嗜酸性白血球及 IgE 為主要標的。
Omalizumab:
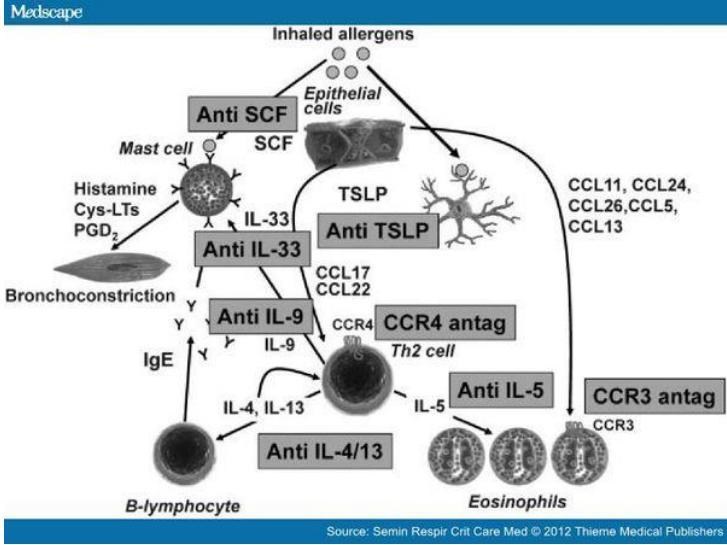
◆IgE的單株抗體可抑制IgE與肥胖細胞結合,但對已經結合在肥胖細胞上的IgE也不會活化之,因此不會誘導肥大細胞產生去顆粒作用
◆ 使用IgE的單株抗體10週後,血清中的IgE明顯降低到測不到濃度,而抗原引起的支氣管痙攣反應也會明顯減少
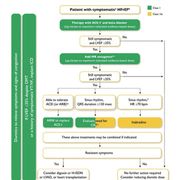
◆Omalizumab treatment reduced exacerbations requiring hospitalization by88% (減少氣喘惡化住院的比率) >these benefits justify the high cost of this treatment in selected individuals with severe disease characterized by frequent exacerbations(由於其價格昂貴,因此選擇性的用在症狀嚴重且惡化頻率高的病人)2017 年底就有許多學者以整合性的照護臨床路徑(integrated care pathways,ICPs)將嚴重過敏性氣喘及嗜酸性粒細胞高的病人制定治療流程,以便臨床醫師參考:
(1)過敏性嚴重氣喘患者,如果總 IgE 是符合使用 Omalizumab 的治療建議範圍時,先使用 Omalizumab 治療 16 周,之後評估治療反應。如果反應有效,就繼續治療。
(2)如果治療無效,就看病人的 eosinophil counts,若高,就改成anti-IL-5 agents 治療。
(3)反之,若病人的 IgE 不高,eosinophil counts 高的病人,就直接使用 anti-IL-5 agents 治療,療程為一年,之後再評估臨床效果。If有療效,就繼續使用 anti-IL-5 agents。
Ref: Lange Basic & Clinical Pharmacology 15th Edition
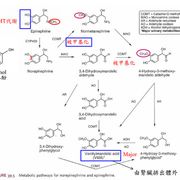
萊豬?萊克多巴胺就是乙型交感神經非選擇作用劑!
Ref:DOI: 10.1111/j.2042-7158.1991.tb03192.x
蘇偉碩花了一堆時間,講了一種叫做DES的賀爾蒙製劑對人體產生的風險跟危害。然後再講狂牛症對人體產生的危害。但我們今天是在講萊克多巴胺啊!!今天A風險高,所以你就要推論B的風險也會高,這是可以這樣推論的嗎?
蘇偉碩還扯了一堆研究,其中一個研究,之前都已經被公開打臉過了,蘇還是硬要講,結果姜醫師回說那個論文他已經看過了,數字根本寫錯了。
很多人說美國人吃美牛美豬都沒事,蘇再鬼扯美國人平均壽命不超過80歲,比台灣人還低。
這種去脈絡化根本無根據沒回顧性研究的鬼扯可以從醫師口中說出,滑天下之大稽!
然後蘇偉碩又拿出一堆高劑量下的動物實驗說會產生細胞或動物的危害。這之前講過一萬次了,那是很高的劑量,而且是觀察性的實驗,講任何毒理問題,請討論劑量!
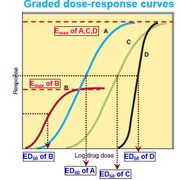
不談論ED50/EC50跟場外藥學大師一樣鬼扯,可笑!
姜醫師今天提到一個重點,有些人說吃萊豬一天吃幾公斤就會超標,但是超標不代表中毒。你如果要吃到中毒,你要吃比這個好幾公斤還更高10倍的量,而且要連續吃。到底誰有辦法吃到這種量?
臺大醫學院毒理學教授腎臟科姜志剛醫師對蘇提出質疑,在牛跟豬裡面的萊克多巴胺都是一樣的東西,為什麼只提案反萊豬,而不反萊牛?
蘇偉碩的回答居然是,因為 國民黨跟民進黨都不反對萊牛, 所以就不提案。而且態度看起來非常理所當然…
你講半天不是一直在講萊劑很可怕、有問題、低劑量也會有風險、還會禍延三代子孫(雖然已上說法都不被醫學界認同),結果你因為兩黨都不反對萊牛,你就只提萊豬公投?
所以你堅持的根本也不是什麼保護民眾健康啊…另外,兩黨都不反對萊牛,所以你就不提案反對。但國民黨跟共產黨現在反對萊豬,你就提案反對。那現在你是堅定支持科學,還是你堅定支持的是國民黨跟共產黨?
完全傻眼,你真的知道自己在公鯊小朋友嗎?這種被榮總開除的國民黨滯台病毒國咖還能繼續有舞台甚至違反醫學倫理鬼扯,真是吾輩之恥!噁心!